10 Types of Anxiety Disorders

Table of content

Anxiety disorder is a group of mental health conditions characterized by overwhelming worrying, fear, anxiety, nervousness, and panic. People with anxiety disorder experience physical and psychological reactions when exposed to a trigger of their symptoms. The trigger depends on the type of anxiety disorder. For a person with a phobia, it can be a situation or event, whereas, for an individual with PTSD, it is any setting or event that reminds a person of trauma they experienced.
Anxiety disorder is not a single, standalone disease. There are many types of anxiety disorders. Different kinds of anxiety disorders are listed below:
- Obsessive-compulsive disorder (OCD)
- Generalized anxiety disorder
- Post-traumatic stress disorder (PTSD)
- Phobia
- Panic disorder
- Separation anxiety disorder
- Agoraphobia
- Social anxiety disorder
- Selective mutism
- Medication-induced anxiety disorder
1. Obsessive-compulsive disorder (OCD)
Obsessive-compulsive disorder (OCD) is a mental health condition where a person has unwanted, recurring thoughts (obsessions) and compulsive behaviors (compulsions). Obsessions become more intense when a person tries to ignore them, and the only way to make those thoughts go away is to perform a compulsion. Upon the completion of compulsive behavior, the relief is temporary, meaning the obsessions keep coming back, thus creating a vicious cycle of OCD. Obsessions and compulsions interfere with daily activities and social interactions, according to the American Psychiatric Association. The obsessive-compulsive disorder tends to center around specific themes such as fear of germs and being contaminated.
Causes of OCD are a combination of abnormalities in brain chemistry or functions, genetics, and learning behavior. When it comes to brain chemistry, abnormalities in the “affective circuit” consisting of a reduced volume in the medial orbitofrontal, anterior cingulate, and temporolimbic cortices are associated with the development of OCD, according to a January 2015 review that F. Piras et al. published in Cortex. The same review showed that the onset of OCD is also associated with tissue expansion in the striatum and thalamus. The authors suggested that OCD mechanisms involve a more widespread network of cerebral dysfunctions than previously thought. For example, they found that besides abnormalities in the “affective circuit,” patients with OCD also have defects in the prefronto-striatal “executive” circuit. Brain areas involved with OCD participate in functions such as motivation and social and emotional behavior. That means dysfunctions in these regions could affect how people behave, regulate emotions, and make decisions.
Besides brain abnormalities, genetics is one of the causes of obsessive-compulsive disorder. The October 2021 paper, by B. Mahjani et al, from Psychological Medicine, confirmed that OCD is a heritable, polygenic disorder with contributions from common and rare gene variants. Examples of these genes include CYP2D6, CYP2C19, SLC6A4, HTR2A, SLC1A1, DLGAP2, COMT, DRD2, BDNF, and NTRK3. Parents can pass on genes and their mutations to children, which contribute to the development of OCD.
Obsessive-compulsive disorder can occur due to learned behavior. Obsessions and compulsions can be learned by watching family members, according to Mayo Clinic.
The main symptoms of OCD are obsessions and compulsions. A person with OCD may be aware these symptoms are problematic, but they can’t ignore obsessions or avoid compulsive behaviors. Obsessions manifest themselves through symptoms such as fear of being contaminated by touching objects that other people have touched, intense stress and anxiety when objects aren’t arranged in a specific order, doubt that you’ve locked the door or turned off the iron or stove, images of driving a car into a crowd of people, unpleasant sexual images, and avoidance of situations that trigger obsessions. Compulsive behaviors occur as symptoms such as constant hand washing, checking the door or stove repeatedly, counting in specific patterns, repeating a prayer or phrase, and arranging objects at home in a certain way.
Risk factors for OCD include a family history of this disorder, stressful life events, and other mental illnesses such as depression, substance abuse, tic disorders (e.g., Tourette syndrome), and anxiety disorders. Results of a nationwide three-generation study by H.C. Steinhausen et al. from the December 2013 issue of Depression and Anxiety showed that having a mother, father, sibling, or offspring with the disorder increases the risk of OCD. Other risk factors include maternal age above 35, male sex by tendency, and ascending year of birth. In a study by P.M.F. de Barros et al. in the January 2021 issue of the European Child and Adolescent Psychiatry, predictors for obsessive-compulsive symptoms are lower socioeconomic status, lower intelligence quotient, higher maternal stress levels during pregnancy, and absence of breastfeeding.
Treatments for OCD are a combination of psychotherapy and medications such as antidepressants. When it comes to therapy, cognitive-behavioral therapy (CBT) is helpful for patients with this disorder.
The main objective of CBT is to help patients identify irrational thoughts and replace them with more rational alternatives, thereby reducing the severity of symptoms such as obsessions and compulsions. What CBT sessions do is that they teach a patient to control their OCD more successfully. A paper that A. Gragnani et al. published in the May 2022 issue of the Journal of Clinical Medicine confirmed the relevance and effectiveness of CBT for patients with OCD emphasizing its potential to improve symptoms and lead to a positive outcome. Therapists may rely on exposure and response prevention (ERP), a form of CBT that involves gradually exposing a patient to a feared object or obsession. The purpose is to help a patient learn ways to resist the urge to perform compulsions.
In addition to medications and therapy, a healthcare professional may recommend other treatment options, such as intensive outpatient and residential treatment programs, deep brain stimulation, and transcranial magnetic stimulation.
Diagnosis of OCD involves a physical exam and psychiatric evaluation. In order to diagnose OCD, a mental health professional uses the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) by the American Psychiatric Association to make sure the patient meets diagnostic criteria. Diagnostic criteria for OCD include the presence of obsessions, compulsions, or both, which are time-consuming and cause significant distress or impairment in social and occupational functioning. Other DSM-5 criteria for OCD include symptoms that aren’t attributable to the physiological effects of a substance (medications or drugs of abuse) or a medical condition, and disturbance isn’t better explained by another mental disorder such as body dysmorphic disorder, eating disorder, and generalized anxiety disorder.
Obsessive-compulsive disorder is common, and it affects 1.6% to 2.3% of the general U.S. population, according to Cleveland Clinic. Past-year prevalence of OCD in U.S. adults is estimated at 1.2% and it was higher in women (1.8%) than men (0.5%), according to a report by the National Institute of Mental Health. The same report showed the lifetime prevalence of OCD in U.S. adults was 2.3%.
2. Generalized anxiety disorder
Generalized anxiety disorder (GAD) is a mental illness characterized by excessive worry regarding everyday situations and issues. A person with GAD worries about many things, not just one. Children and adults can develop GAD, and it can co-occur with psychiatric conditions such as depression, panic disorder, specific phobia, and social anxiety disorder. It begins in childhood or adolescence, but people of all ages can develop GAD.
Causes of GAD are biological and environmental factors such as differences in brain function and structure, genetics, differences in perception of threats, and development and personality. Generalized anxiety disorder is associated with significant anatomical changes in the brain, especially in areas associated with anxiety neurocircuitry. For instance, patients with GAD tend to have an increased grey matter volume in the amygdala (regulates emotional processes and fearful/threatening stimuli), increased cortical thickness in the right inferolateral and ventromedial prefrontal cortex (PFC), the left inferior and middle temporal cortex, and right lateral occipital cortex, according to a June 2017 paper in Dialogues in Clinical Neuroscience published by Dr. Eduard Maron and Dr. David Nutt of Imperial College London.
The same paper suggested that GAD is associated with reduced hippocampal volume, and it has a heritability of 32% up to 49%. Genes implicated in the development of GAD include MAOA and SLC6A4. More precisely, changes in brain areas involved in emotions and processing of fearful or threatening stimuli and thoughts and actions can contribute to the onset of generalized anxiety disorder. Parents can also pass on genes and their variants to children, which makes genetics an important aspect of the development of GAD.
Symptoms of GAD can vary, but they usually include persistent worrying and anxiety about everyday situations that are out of proportion to the impact of events, overthinking plans and solutions, perceiving events/situations as threatening even though they’re not, inability to stop worrying, indecisiveness and fear of making wrong decisions, restlessness, difficulty relaxing, feeling on edge, and difficulty concentrating. Besides physiological symptoms, people with GAD also have physical responses such as trouble sleeping, fatigue, muscle tension/ache, trembling, nervousness, irritability, sweating, nausea, diarrhea, or irritable bowel syndrome, according to Mayo Clinic.
Risk factors for GAD are family history of GAD, history of major life changes or childhood trauma, and recent traumatic or negative events. People with chronic medical illnesses and mental disorders are also more susceptible to GAD. Timid or negative personality or avoiding anything dangerous are also risk factors for generalized anxiety disorders. Other factors associated with GAD are female gender, unmarried, poor health, presence of stressors, and low education, according to Dr. Sadaf Munir and Dr. Veronica Takov of McLaren Macomb Regional Medical Center in their post published by the National Library of Medicine. Excessive tobacco and caffeine use is also a risk factor for GAD because it worsens anxiety, Healthline explained.
Treatments for GAD are psychotherapy and medications or a combination of both. The most effective type of psychotherapy for the treatment of GAD is cognitive-behavioral therapy, according to Mayo Clinic. The goal of CBT is to teach patients skills that help them manage their worries so they can return to activities they avoided due to anxiety. With CBT sessions, people learn to identify irrational thoughts and adopt a rational thinking pattern, thereby reducing their symptoms. CBT is the first-line treatment for GAD and it is particularly effective when the focus is on targeting cognitive processes that maintain worry, as per C. R. Hirsch et al. in their paper from the November 2019 issue of Frontiers in Psychiatry.
When it comes to medications, doctors usually prescribe antidepressants such as paroxetine (Paxil), escitalopram (Lexapro), venlafaxine (Effexor XR), or duloxetine (Cymbalta). Besides antidepressants, a healthcare professional may prescribe anti-anxiety medications such as buspirone (Buspar) and benzodiazepines. Antidepressants and anti-anxiety medications reduce the severity of symptoms, but it can take several weeks for them to work. Benzodiazepines are prescribed for short-term use only because they are habit-forming.
Generalized anxiety disorder is diagnosed after a physical exam and psychiatric evaluation. A physical exam is performed to check whether the symptoms are a side effect of medications or associated with an underlying medical condition. The doctor may order a blood test and urine test. Psychiatric evaluation involves checking a patient’s medical history and asking questions about their symptoms. Patients may need to complete a questionnaire that informs a psychiatrist about their thinking patterns and behaviors.
The doctor diagnoses GAD if a patient meets the diagnostic criteria from DSM-5. Diagnostic criteria include anxiety and worry about a variety of topics and activities, worry is challenging to control, and anxiety/worry is accompanied by at least three of six physical symptoms (restlessness/edginess, tiring easily, poor concentration, irritability, muscle ache/soreness, and difficulty sleeping). In order to be diagnosed with GAD, a patient needs to experience excessive worry or anxiety on most days than not for at least six months.
Generalized anxiety disorder is a common mental illness with a past-year prevalence of 2.7% among U.S. adults, according to the National Institute of Mental Health. Past-year prevalence was higher in women (3.4%) than in men (1.9%). The lifetime prevalence of GAD is 5.7% in U.S. adults and 2.2% in adolescents.
3. Post-traumatic stress disorder (PTSD)
Post-traumatic stress disorder (PTSD) is a mental health condition that develops after a traumatic event that a person has experienced or witnessed. Examples of traumatic events include accidents, fire, war, natural disasters, physical or sexual abuse, terrorist attack, and the death of a loved one. People who experience traumatic events, or witness them, experience difficulties coping, but they get better with time and good self-care. However, symptoms may persist and trigger uncontrollable thoughts about trauma and anxiety to the point it affects a person’s quality of life. That means a person may have PTSD.
The causes that contribute to the development of PTSD are unclear because not all people who experience or witness trauma get this mental condition. A combination of different causes could be involved, such as the severity of the trauma, inherited mental risks, temperament, and how the brain regulates chemicals and hormones released as a response to stress. Genetics also plays a role in the development of PTSD. In fact, genetic factors account for 30% to 40% of the heritability of this disorder, according to a paper by S.B. Banerjee et al. in a paper from the May 2017 issue of Neuroscience Letters.
People with PTSD have alterations in brain areas associated with stress response, according to a study by Dr. J. Douglas Bremner of Emory University School of Medicine published in the December 2006 issue of Dialogues in Clinical Neuroscience. These areas are the amygdala, hippocampus, and prefrontal cortex. The alterations are also observed in neurochemical stress response systems, including stress hormones cortisol and norepinephrine. When it comes to stress hormones, it’s useful to mention that a lack of baseline cortisol at the time of trauma could facilitate the overactivation of central corticotropin-releasing hormone and norepinephrine (CRH-NE) cascade, thereby enhancing and prolonging stress response, according to a paper by Dr. Jonathan E. Sherin and Dr. Charles B. Nemeroff of Leonard M. Miller School of Medicine published in September 2011 issue of Dialogues in Clinical Neuroscience. This is important because CRH is the central regulator of the hypothalamic-pituitary-adrenal (HPA) axis, which is crucial for stress response.
The above mentioned studies indicate that genetic predisposition and abnormalities in the brain’s structure and function are major components in the onset of PTSD. Changes in brain structure and levels of stress hormones can affect how people think, behave, and react under stress.
Symptoms of PTSD vary from person to person, but they usually include avoiding things or situations that remind them of a traumatic event, difficulty relaxing or being “on edge”, negative thoughts and feelings such as feeling angry, guilty, distrustful, and reliving or re-experiencing the traumatic event. The symptoms start within one month of a traumatic event, but it’s also possible for them to appear years later. People also experience changes in physical and emotional reactions e.g., they’re easily scared and are always on guard for danger.
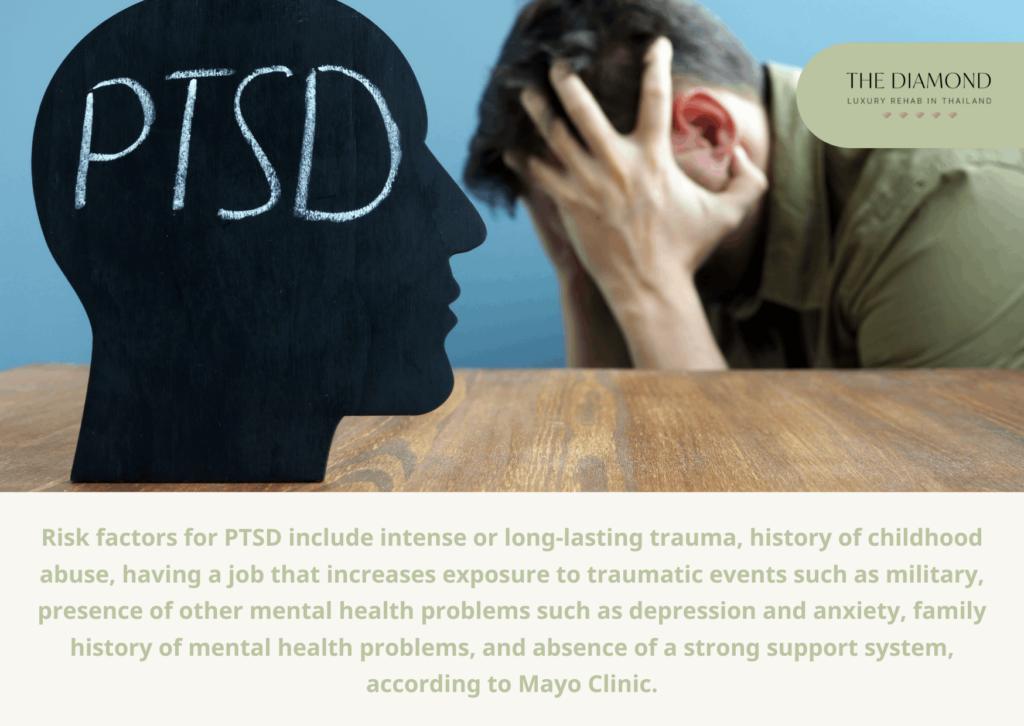
Risk factors for PTSD include intense or long-lasting trauma, history of childhood abuse, having a job that increases exposure to traumatic events such as military, presence of other mental health problems such as depression and anxiety, family history of mental health problems, and absence of a strong support system, according to Mayo Clinic.
Treatments for PTSD include psychotherapy and medications. A therapist relies on different types of therapy when treating patients with PTSD, such as cognitive processing therapy, prolonged exposure therapy, and eye movement desensitization and reprocessing (EMDR). The main purpose of cognitive therapy is to help a patient identify negative thoughts and beliefs about the traumatic event and change them. Exposure therapy encourages a person to face their thoughts, feelings, and situations they’ve been avoiding. Finally, EMDR aims to make the traumatic event less upsetting over time by having a patient focus on specific movements or sounds that a therapist introduces while they’re thinking about the event. What makes prolonged exposure therapy, trauma-focused CBT, and cognitive processing therapy effective is that they directly address memories of traumatic events or thoughts and feelings related to them, according to a paper by L.E. Watkins et al. in November 2018 issue of Frontiers in Behavioral Neuroscience.
Medications used in the treatment of PTSD include antidepressants to help with symptoms of depression and anxiety and anti-anxiety medications to alleviate severe anxiety.
Diagnosis of PTSD includes a physical exam to check for the presence of medical problems that cause symptoms and psychological evaluation. During the psychological evaluation, a psychiatrist discusses symptoms and traumatic events that triggered them. They will diagnose PTSD if a patient meets the diagnostic criteria from DSM-5. Diagnostic criteria for PTSD include exposure to the traumatic event, one or more intrusion symptoms, one or more symptoms of avoidance, two or more symptoms of negative changes in feelings and mood, and two or more symptoms of changes in reactivity or arousal. In order to meet diagnostic criteria, these symptoms need to last longer than a month, not be due to substance abuse or a medical condition and induce significant distress to a person’s quality of life.
Post-traumatic stress disorder is a common mental illness with a lifetime prevalence of 6.8% and a past-year prevalence of 3.6% among U.S. adults, according to the National Institute of Mental Health. The same report showed that past-year prevalence was higher in women (5.2%) than in men (1.8%). Prevalence of PTSD in adolescents is 5.0%. Cleveland Clinic reports that at least half of people in the U.S. have experienced a traumatic event and 10% of men and 20% of women from that group develop PTSD.
4. Phobia
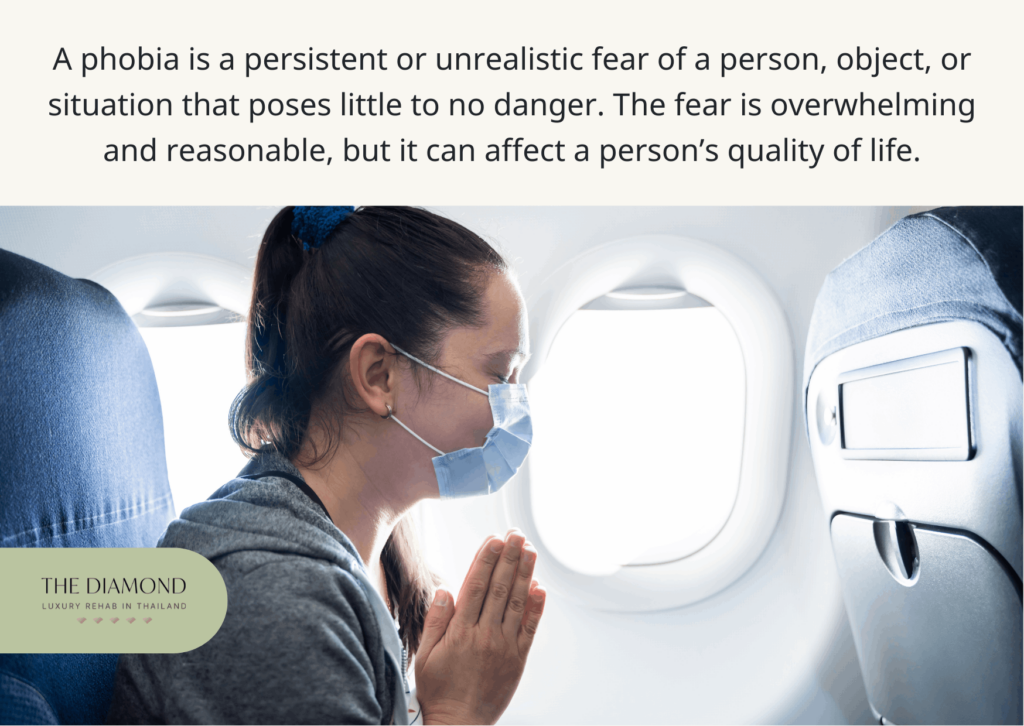
A phobia is a persistent or unrealistic fear of a person, object, or situation that poses little to no danger. The fear is overwhelming and reasonable, but it can affect a person’s quality of life. Known as a specific phobia, this mental condition is long-lasting. Phobia and fear aren’t the same things. Fear is a rational reaction to a potentially dangerous situation or object, but phobia is an irrational fear i.e., a fear response even when a person isn’t in danger. Categories of specific phobias are situational, nature, animals, blood and injection or injury, and others such as vomiting. Examples of phobias are acrophobia (fear of heights), arachnophobia (fear of spiders), cynophobia (fear of dogs), and astraphobia (fear of storms).
Causes of phobia include negative experiences or panic attacks related to a specific situation/object, changes in brain functioning, and genetics. A phobia can also be a learned behavior because a person can learn fear or anxiety from someone in their environment, such as parents or siblings. Specific phobias are moderately heritable, especially animal-related phobias, according to a review by C.M.H.H. van Houtem et al. in the May 2013 issue of the Journal of Anxiety Disorders. That means a person may have a genetic predisposition that makes them more vulnerable and susceptible to phobia. Phobias are linked to significant alterations in brain activity, including increased activity of the amygdala during exposure to phobia-inducing stimuli. Changes in brain areas such as stria terminalis, anterior cingulate cortex, and the insula are also associated with a phobia, according to Dr. Heidi Moawad’s post on Neurology Live. These brain areas play a role in behavioral responses and emotion regulation.
Symptoms of phobia can be physical and psychological. The latter include impending doom feeling, intense discomfort, an urge to escape, a sense of losing control, and depersonalization (a sense of things being unreal). Physical symptoms of phobia are heart palpitations, shaking, sweating, hot flushes or chills, shortness of breath, chest pain, nausea, dizziness, fainting, and lightheadedness. These symptoms occur when a person is exposed to the object of their phobia or when they anticipate it.
Risk factors for phobia include age, family history of specific phobia, sensitive and more inhibited temperament, experiencing a traumatic event associated with the object of phobia, and learning about negative experiences such as hearing news about a plane crash. Specific phobias tend to appear in childhood, usually by the age of 10, but people can develop them in adulthood, according to Mayo Clinic.
Treatments for phobia include psychotherapy and medications. The best types of psychotherapy for people with a phobia are exposure therapy and CBT. The main objective of exposure therapy is to change a patient’s response to the feared object or situation through gradual, repeated exposure in a controlled setting under the therapist’s supervision and guidance. On the flip side, CBT helps patients cope with feared objects or situations in a healthier manner. It emphasizes learning to develop more confidence with thoughts and feelings instead of being overwhelmed by them. A rapid review by C.E.W. Thng et al. in the March 2020 issue of F1000Research reported that exposure therapy is an empirically supported and widely accepted treatment for phobia and also confirmed CBT can help alleviate symptoms.
Diagnosis of a specific phobia relies on a thorough clinical interview during psychological evaluation. A psychiatrist diagnoses phobia when a patient meets DSM-5 criteria. Diagnostic criteria include unreasonable, excessive fear, immediate anxiety response, avoidance or extreme distress, significant impact on life, duration of symptoms at least six months, and symptoms that are not better explained by other conditions such as OCD.
A phobia is a relatively common anxiety disorder with a lifetime prevalence of 12.5% and a past-year prevalence of 9.1% among U.S. adults. Past-year prevalence of phobia is higher in women (12.2%) than men (5.8%). The lifetime prevalence of phobia in U.S. adolescents is 19.3%, according to the National Institute of Mental Health.
5. Panic disorder
Panic disorder is a mental health condition characterized by regular and sudden panic attacks. A person with panic disorder is in constant fear of having another panic attack. The main difference between a panic disorder and a panic attack is that the latter is a sudden episode of intense fear that goes away when a stressful situation ends. Panic disorder is recurrent.
Causes of panic disorder are genetics, major life stress, changes in brain function, and a temperament that is more vulnerable to stress or prone to negative emotions. Several genes are implicated in the onset of panic disorder. These genes include NPY, ADORA2A, COMT, IKBKE, NPY5R, BDKRB2, and SLC6a2, according to a paper that Dr. Eun Jeong Kim and Dr. Yong-Ku Kim of the Korea University Ansan Hospital published in July 2018 issue of AIMS Genetics. Panic disorder is associated with various structural and functional changes in brain areas such as the amygdala and hippocampus, HPA axis, according to a study by Dr. Fiammetta Cosci and Dr. Giovanni Manseuto of the University of Florence in the January 2019 issue of Psychiatry Investigation. These brain areas modulate response to fear and stress.
Symptoms of panic disorder are anxiety or feeling of unease, worry, and fear that leads to panic attacks. Signs and symptoms of a panic attack are a racing heartbeat, feeling faint, nausea, chest pain, trembling, shortness of breath, sweating, chills or hot flushes, dizziness, choking sensation, pins, and needles sensation, ringing in the ears, abdominal cramping, and feeling of unreality.
Risk factors for panic disorder are a family history of panic disorder, major life stress, traumatic event, major changes in life, history of childhood physical or sexual abuse, and smoking or taking too much caffeine, according to Mayo Clinic.
Treatments for panic disorder are psychotherapy and medications. People with panic disorder can benefit from CBT as it helps them learn through their experience that panic symptoms aren’t dangerous. Additionally, CBT teaches patients to recognize that their thoughts are irrational so they can replace them with more realistic alternatives. CBT techniques such as cognitive restructuring and interoceptive exposure are particularly effective in the treatment of the panic disorder, according to a study by A. Pompoli et al. in the September 2018 issue of Psychological Medicine.
Medications for the treatment of panic disorder are prescribed to reduce symptoms of panic attacks and manage depression. These medications include antidepressants such as selective serotonin reuptake inhibitors (SSRIs), serotonin and norepinephrine reuptake inhibitors (SNRIs), and sedatives such as benzodiazepines.
Diagnosis of the panic disorder requires a physical exam that includes blood and urine tests and psychiatric evaluation. The healthcare professional performs thorough evaluations to determine whether a patient has a panic attack, panic disorder, or a medical condition. They will diagnose panic disorder when a patient meets the criteria from DSM-5. Diagnostic criteria for panic disorder include frequent and unexpected panic attacks, at least one of the attacks has been followed by one month or more of ongoing worry about another panic attack, and panic attacks aren’t caused by substance abuse, medical condition, or mental illness such as a phobia.
Panic disorder is a relatively common mental illness with a lifetime prevalence of 4.7% and a past-year prevalence of 2.7% among U.S. adults. Past-year prevalence is higher in women (3.8%) than in men (1.6%). The lifetime prevalence of panic disorder in U.S. adolescents is 2.3%, according to the National Institute of Mental Health.
6. Separation anxiety disorder
Separation anxiety disorder is a mental condition characterized by an intense fear of being separated from a loved one. Although separation anxiety is a normal stage of a child’s development that they grow out of, separation anxiety disorder is a more serious condition that starts as early as preschool age. Adults can develop a separation anxiety disorder, too.
Causes of separation anxiety disorder can be genetics and environmental factors, including death in the family, separation or divorce of parents, parental absence, parental anxiety or alcoholism, and adoption or foster care. The condition tends to run in families, which implies it could have a genetic component. Moreover, shared genetic determinants are a major underlying cause of the developmental continuity of childhood separation anxiety disorder into adult panic disorder, according to a study by M. Battaglia et al. in the January 2009 issue of the Archives of General Psychiatry. These findings indicate both disorders have a genetic component.
Symptoms of a separation anxiety disorder include temper tantrums when a parent leaves, fear that something bad would happen to a family member during separation, fear of getting lost or being abducted, fear of being left alone, following a caregiver around the house, bedwetting, and nightmares. A child with a separation anxiety disorder may refuse to sleep in their own bed because they want to sleep with their parents. Patients with this disorder can experience physical reactions such as headaches, stomach aches, dizziness, nausea, vomiting, difficulty breathing, and diarrhea when separated from a loved one.
Risk factors for separation anxiety disorder are life stress or loss that results in separation e.g. death of a family member, family history of anxiety, environmental issues such as disasters that result in separation, big life changes such as moving to a different town or changing school, and strict parental upbringing. Other risk factors include shy or timid personality, low socioeconomic status, overprotective parents, a lack of appropriate parental interaction, and having problems dealing with kids of their own age, according to Healthline.
Treatments for separation anxiety disorder include psychotherapy and medications such as SSRIs. According to Mayo Clinic, patients with separation anxiety disorder can benefit from CBT, which teaches them to face and manage fears about separation. Parents can benefit from CBT, too, because they learn how to provide emotional support and encourage a child to be independent. Medications are prescribed to adult patients with separation anxiety disorder.
Diagnosis of separation anxiety disorder in children is made by observing a child in a scene of separation and assessing their medical history and symptoms. Diagnosis of separation anxiety disorder in adults is made through a psychological evaluation. A psychiatrist diagnoses separation anxiety disorder when a child or adult meets the criteria from DSM-5.
Diagnostic criteria for separation anxiety disorder include inappropriate or excessive fear or anxiety concerning separation from the attachment figure, as evidenced by at least three of eight symptoms. These symptoms include recurrent excessive distress when anticipating separation, persistent worry about losing attachment figure, worry about an event that may cause separation, refusal to go out due to fear of separation, excessive fear of being alone, refusal to sleep away from home, repeated nightmares involving separation, and physical symptoms. Other diagnostic criteria are that symptoms last at least four weeks in children and six months in adults, the symptoms cause significant distress in everyday life, and disturbance is not better explained by another mental disorder such as agoraphobia.
Separation anxiety disorder is more common than people believe, with 4% prevalence in population-based studies, with an increase to 7.6% of pediatric patients in a clinical setting, according to a post by J. Feriante et al. on the website of National Library of Medicine.
7. Agoraphobia
Agoraphobia is a mental condition characterized by fear of places and situations from which it would be difficult to escape or receive help. A person with agoraphobia avoids places that cause anxiety and fear, such as public and crowded places. People may fear an actual or upcoming situation. Agoraphobia is different from specific phobias because the latter is centered on harm directly caused by the situation, whereas agoraphobia focuses on whether escape is possible.
The causes of agoraphobia are still unclear but are associated with genetics, learning experiences, and existing conditions such as depression and panic disorder. Genetic predisposition in agoraphobia was confirmed in older studies such as a paper by R.R. Crowe from the summer 1985 issue of Psychiatric Developments. More research is necessary to elucidate all causes of agoraphobia and its mechanisms.
Symptoms of agoraphobia include fear of leaving home alone, using public transportation, and being afraid of enclosed or open spaces. These situations cause significant stress and anxiety, which is why people with agoraphobia tend to avoid them. They may also experience physical symptoms such as rapid heart rate, chest pain, hyperventilation, lightheadedness or dizziness, sudden chills or flushing, excessive sweating, upset stomach or diarrhea, and feeling shaky, numb, or tingling.
Risk factors for agoraphobia include a personal history of panic attacks and specific phobias, anxious or nervous personality, responding to panic attacks with avoidance and excessive fear, a history of stressful life events and trauma, and a family history of agoraphobia, according to Mayo Clinic.
Treatments for agoraphobia include psychotherapy and medications such as antidepressants and anti-anxiety medications. Therapy is the first-line treatment for agoraphobia because it helps a patient work through their fears. A CBT therapist empowers a patient to recognize thoughts that cause anxiety. The patient then learns ways to react in a healthier and better way. In a case study reported by Dr. Naeem Aslam of the Quaid-i-Azam University from Pakistan in the January-March 2012 issue of the Indian Journal of Psychological Medicine, a 24-year-old patient with agoraphobia experienced improvements, and his symptoms diminished after seven CBT sessions.
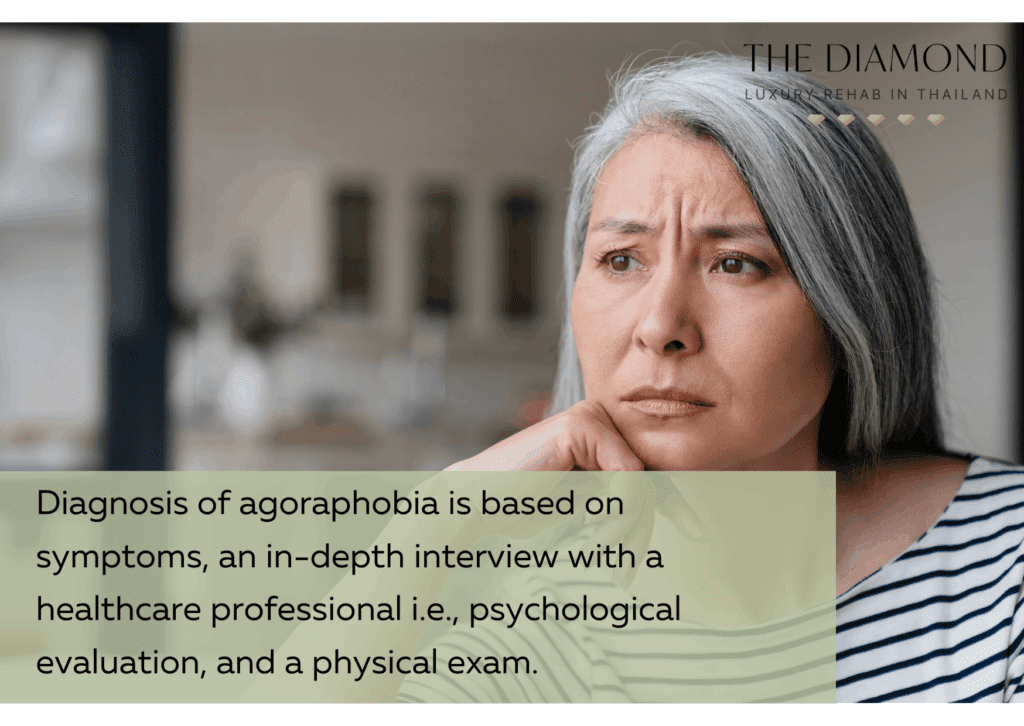
Diagnosis of agoraphobia is based on symptoms, an in-depth interview with a healthcare professional i.e., psychological evaluation, and a physical exam. The psychiatrist or psychologist diagnoses agoraphobia when a patient meets the criteria from DSM-5. Diagnostic criteria indicate that fear of at least two of five situations must be present such as using public transportation, being in open spaces, being in enclosed spaces, being in crowds or a line, and being outside the home. This fear should be present for at least six months to meet DSM-5 diagnostic criteria. Other criteria indicate that the same situations always trigger anxiety, patients actively avoid the situation or request the presence of a companion, fear is out of proportion to the actual threat, and fear causes significant distress on quality of life.
Agoraphobia is not as common as other anxiety disorders, such as GAD. The lifetime prevalence of agoraphobia in U.S. adults is 1.3%, and the past-year prevalence is 0.9%. The past-year prevalence is almost similar in women (0.9%) and men (0.8%). The lifetime prevalence of agoraphobia in U.S. adolescents is 2.4%, according to the National Institute of Mental Health.
8. Social anxiety disorder
Social anxiety disorder, or social phobia, is a mental condition indicated by an overwhelming fear of social situations. A person with social anxiety disorder fears they will be criticized, judged, embarrassed, or humiliated in social situations such as public speaking. Intense anxiety can lead to avoidance of that specific situation.
The causes of social anxiety disorder are genetics, changes in brain structure, and environment. The latter refers to social anxiety disorder as a learned behavior that occurs after an embarrassing social situation. When it comes to genetics, DNA methylation may play a role in biological mechanisms of social anxiety disorder, according to a study that A. Wiegand et al. published in the February 2021 issue of Translational Psychiatry. The study identified two differently methylated areas linked to this disorder within genes SLC43A2 and TNXB. The term DNA methylation refers to a chemical reaction that regulates gene expression. Brain abnormalities in social anxiety disorder involve hyperactivation of the fear circuit consisting of the amygdala, insula, prefrontal cortex, and anterior cingulate cortex, according to a paper by Dr. Janna Marie Bas-Hoogendam and Dr. P. Michiel Westenberg of Leiden University Medical Center in April 2020 issue of F1000Research.
Symptoms of social anxiety disorder can be emotional or behavioral, physical, and avoidance of common social situations. Emotional and behavioral symptoms include fear of situations where a person may be judged negatively, worry about being humiliated or embarrassed, fear that people will notice anxiety, fear of physical symptoms, anxiety in anticipation of a specific social situation, avoidance of situations that trigger anxiety, and overthinking to identify flaws in your interactions.
Physical symptoms of a social anxiety disorder include a fast heartbeat, blushing, sweating, trembling, nausea or upset stomach, shortness of breath, dizziness, muscle tension, and feeling that the mind has become blank. Avoidance of social situations refers to situations such as interacting with unfamiliar people, going to school, attending social gatherings, making eye contact, starting conversations, dating, and using a public restroom.
Risk factors for social anxiety disorder include a family history of this disorder and negative experiences in childhood, such as bullying, teasing, ridicule, rejection, humiliation, trauma, abuse, and family conflict. Other risk factors include a shy or timid personality, new social or work demands such as public speaking, and having an appearance or condition that draws attention, such as facial disfigurement or Parkinson’s disease.
Treatments for social anxiety disorder are psychotherapy and medications. According to Mayo Clinic, the most effective type of therapy for patients with a social anxiety disorder is CBT, especially exposure-based CBT. During therapy sessions, patients gradually work up to facing situations they fear the most. With CBT, patients can improve coping skills and learn to address the trigger of their anxiety in a healthy manner. They also learn to identify unrealistic thoughts and replace them with realistic alternatives, thereby reducing the severity of their anxiety.
Medications are used in combination with therapy, and they usually include SSRIs such as paroxetine (Paxil) and sertraline (Zoloft) or SNRIs such as venlafaxine (Effexor XR). In addition to these medications, patients with a social anxiety disorder may receive anti-anxiety medications and beta blockers to reduce the intensity of their physical symptoms.
Diagnosis of social anxiety disorder includes a physical exam and psychological evaluation. The condition is diagnosed when a patient meets the diagnostic criteria from DSM-5. These criteria include persistent or intense fear or anxiety about specific social situations because a person believes they may be judged negatively, avoidance of anxiety-inducing situations, anxiety is out of proportion to the situation, symptoms interfere with daily life, and anxiety is not better explained by substance abuse or medical condition.
Social anxiety disorder is a common mental condition with a lifetime prevalence of 12.1% and a past-year prevalence of 7.1% among U.S. adults. Past-year prevalence is higher in women (8.0%) than in men (6.1%). The lifetime prevalence of social anxiety disorder in U.S. adolescents is 9.1%, according to the National Institute of Mental Health.
9. Selective mutism
Selective mutism is a mental condition indicated by the inability to speak in certain social situations, such as with strangers. A person with selective mutism doesn’t refuse to speak; they are simply not able to do so. Selective mutism affects children, but adults can have it as well.
The causes of selective mutism are unclear because the condition is rare. Potential causes of selective mutism are childhood abuse, trauma, and upheaval. Selective mutism is associated with social anxiety disorder, and people may have a genetic predisposition to it, according to Very Well Mind.
Symptoms of selective mutism include a significant contrast in the ability to engage with people e.g. being talkative with family and mute with strangers, nervousness or being socially awkward, appearing disinterested or sulky, clingy, shy, or withdrawn behavior, and being stubborn or aggressive. More confident children may use gestures to communicate e.g., shake their head for “no” or nod for “yes”, but children with more severe symptoms don’t communicate verbally or non-verbally.
Risk factors for selective mutism include a shy personality, being an immigrant, personal history of other anxiety disorders such as social anxiety disorder, problems with self-regulation, and fear of being embarrassed in front of others. People with depression, autism spectrum disorder, developmental delays, language problems, OCD, and panic disorder are also at risk for selective mutism.
Treatments for selective mutism include therapy and medications such as antidepressants. Therapy is focused on CBT because it consists of various techniques that help patients overcome triggers of their anxiety. These techniques include desensitization to overcome sensitivity to triggers, exposure therapy, positive reinforcement, and shaping to reward positive behaviors. A study by B. Oerbeck et al. from the January 2018 issue of European Child and Adolescent Psychiatry confirmed the long-term effectiveness of CBT for patients with selective mutism.
Diagnosis of selective mutism involves a thorough evaluation, and a psychiatrist ensures a patient meets diagnostic criteria from DSM-5. In children, the symptoms of selective mutism need to be present for at least one month, a child must understand spoken language and be able to speak normally at home, and a lack of speech must interfere with a child’s educational or social functioning. In adults, the symptoms must be present for at least one month, and they interfere with their functioning as well.
Selective mutism is an uncommon disorder with a prevalence of 1% to 2%, according to a paper by Dr. Christopher A. Kearney and Prof. Melanie Rede of the University of Nevada in the June 2021 issue of Frontiers in Psychology.
10. Medication-induced anxiety disorder
Medication-induced anxiety disorder is a mental condition characterized by anxiety or panic attacks that occur when a person uses or stops using medications or substances such as alcohol and drugs. Although it is normal to experience anxiety during intoxication or withdrawal, this disorder has a significant impact on a person’s life and causes social and functional impairments.
Causes of medication-induced anxiety disorder are the changes in brain chemicals due to the consumption of certain substances or taking medications, according to Tufts Medical Center.
Symptoms of a medication-induced anxiety disorder include feeling worried, nervousness, thinking bad things will happen, difficulty falling asleep and waking up during the night, difficulty concentrating, poor memory, fear of losing control, losing weight, chills, hot flashes, shaking, sweating, fast heartbeat, chest pain, and shortness of breath. The symptoms appear while a person is taking drugs or within a few days after they stop taking them.
Risk factors for medication-induced anxiety disorder are the use of alcohol and illegal drugs such as LSD and cocaine, nonprescription medicines such as decongestants, caffeine, and prescription medications such as steroids, stimulants, and medicines for asthma, Parkinson’s disease, and thyroid problems.
Treatments for medication-induced anxiety disorder include changing medications or treatment of the symptoms. People who abuse alcohol and drugs can overcome this disorder by stopping the use of these substances through addiction recovery, which also relies on therapy such as CBT. Addiction recovery can include inpatient and outpatient programs, depending on the severity of substance abuse. People whose symptoms are due to prescription medications must avoid altering dosage on their own. A healthcare provider should be consulted instead.
Diagnosis for medication-induced anxiety disorder requires a thorough evaluation to ensure whether anxiety was present before the use of drugs or substances. A healthcare professional will diagnose this disorder only when a patient meets the diagnostic criteria from DSM-5. These criteria indicate that symptoms must develop during or within a month of use or intoxication or within a month after withdrawal from drug or substance abuse known to cause anxiety. Symptoms must not be attributed to other anxiety disorders and must not be a result of delirium caused by the drug.
Medication-induced anxiety disorder is uncommon, with a past-year prevalence of 0.002%, according to PsychDB. Prevalence is likely to be much higher, they explained.
What is anxiety disorder?
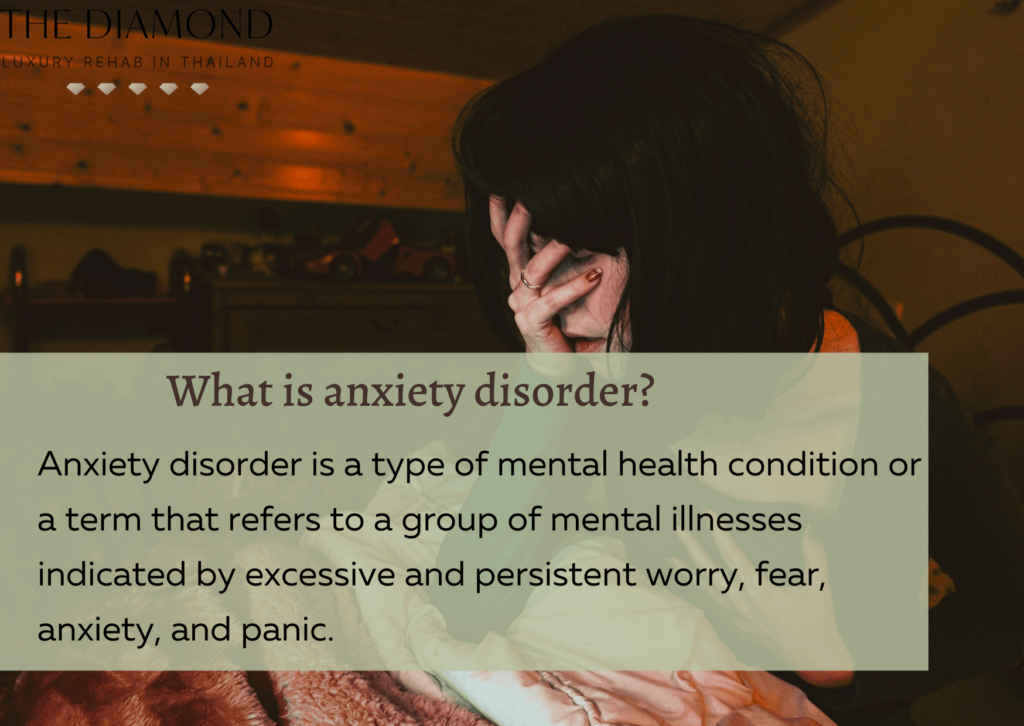
Anxiety disorder is a type of mental health condition or a term that refers to a group of mental illnesses indicated by excessive and persistent worry, fear, anxiety, and panic. Anxiety disorder is not a specific mental illness but a category that includes multiple conditions that have anxiety, fear, worry, or panic in common. According to a paper by B.W. Pennix et al. in the March 2021 issue of The Lancet, anxiety disorders are the most common group of mental disorders, and they usually start before or in early adulthood. These disorders involve dysfunction of brain circuits that respond to danger.
In DSM-5, eleven types of anxiety disorder are described, but in the previous edition (DSM-4), there were 12. In the previous issue, panic disorder and agoraphobia were one condition i.e. a patient could be diagnosed with panic disorder with agoraphobia or without. The latest issue, DSM-5, separates them into two specific conditions.
Anxiety disorder is not a modern-day mental condition. It has been present for centuries. The word anxiety derives from the Latin substantive angor and verb ango meaning to constrict. Anxiety has a long history that stems from ancient times. For instance, The Hippocratic Corpus, a collection of medical texts attributed to Hippocrates or written by disciples in his name, described the phobia of a man called Nicanor. Nicanor was afraid of the flute, and whenever he heard the sign of this instrument, he experienced feelings of terror. His symptoms persisted for a long time. Nicanor’s case is a typical representation of phobia, reported Dr. Marc-Antoine Crocq of Maison des Adolescents du Haut-Rhin in the September 2015 issue of Dialogues in Clinical Neuroscience.
Stoic philosopher Cicero in Tusculan Disputations, wrote that worry, affliction, and anxiety are called disorders that represent the analogy between a diseased body and a troubled mind. In Cicero’s text, anxiety is distinguished from sadness, but it is considered a medical condition.
Between ancient and modern times, it seems that the concept of anxiety has disappeared from written records. While people with anxiety existed during those times, they were diagnosed with other diagnostic terms, such as Beard’s neurasthenia. However, it’s useful to mention one of the most influential works from the middle ages, Robert Burton’s The Anatomy of Melancholy which was published in 1621. The book is an encyclopedic review of literature from ancient times to the 17th century. Although it is widely discussed in terms of depression, it was also concerned with anxiety. In fact, melancholia wasn’t limited to depression only, it also encompassed anxiety.
In the 18th century, medical authors published a description of panic attacks, but they didn’t consider them to be separate illnesses. It was believed panic attacks were symptoms of melancholia. When it came to medical authors in the 18th century, it’s useful to mention Boissier de Sauvages, who published the first significant French medical nosology, which also featured a list of mental disorders, including panophobia. This is important because panophobia is concerned with anxiety and is defined as panic, terror, or fear whose cause is not obvious. Subtypes of panophobia are reminiscent of modern anxiety disorders.
Anxiety was a major component of various diagnostic categories in the 19th and 20th centuries.
In DSM-1, published in 1952, anxiety was synonymous with psychoneurotic disorders. The first edition of DSM stated that the main symptom of psychoneurotic disorders was anxiety, which was interpreted as a danger signal sent and perceived by the conscious aspect of personality.
In DSM-2, published in 1968, the category for anxious symptomatology was named neuroses. This edition of DSM established anxiety and neurosis as quasi-symptoms. However, DSM-3, which was published in 1980, included an anxiety disorder chapter. This chapter included phobic disorders, anxiety states, and PTSD. In DSM-4 from 1994, anxiety disorders were still divided into several subtypes, and acute stress disorder was also introduced. Finally, DSM-5, published in 2013, separated agoraphobia and panic disorder and modified diagnostic criteria for disorders such as selective mutism, which was among childhood and adolescent disorders before.
What is the most common type of anxiety disorder?
The most common type of anxiety disorder is generalized anxiety disorder, Mental Health UK reported. In a study by A.M. Ruscio et al. from the May 2017 issue of JAMA Psychiatry, global lifetime prevalence of DSM-5 GAD was 3.7%, the 12-month prevalence was 1.8%, and the 30-day prevalence was 0.8%. GAD was more common in high-income countries, despite a negative association between this anxiety disorder and socioeconomic status within countries.
For example, in any given week in the UK, 6 out of 100 people have GAD as opposed to 4 in 100 people having PTSD, 2 in 100 people having phobias, and 1 in 100 people having OCD, according to the Priory Group. The American Psychiatric Association reports that specific phobia is the most common in U.S. adults as it affects 8% to 12% of people.
It is not clear why GAD is the most common type of anxiety disorder. However, it can worsen in times of stress such as physical illness, upcoming exams, and family-related problems, according to the National Institute of Mental Health. Since stress is a normal part of life, people may be more prone to GAD, especially if they are vulnerable to it.
How are different types of anxiety disorders identified?
Different types of anxiety disorders are identified based on their symptoms. The process through which anxiety disorders are identified involves diagnostic criteria from DSM-5. While all anxiety disorders share anxiety or worry in common, they have their unique characteristics. Checking DSM-5 diagnostic criteria allows psychologists and psychiatrists to identify the specific type of anxiety disorder a patient may have.
Anxiety disorders are classified into several subtypes such as GAD, panic disorder, social anxiety disorder, and phobia-related disorders, according to the National Institute of Mental Health. As mentioned above, GAD is persistent worry about everyday things, panic disorder involves frequent and sudden panic attacks, whereas social anxiety disorder includes fear of social situations or being judged and humiliated. Phobia-related disorders include specific phobias, agoraphobia, and separation anxiety disorder. Even social anxiety disorder is a type of phobia-related anxiety disorder. What these disorders have in common is fear that patients experience in the presence of triggers of their anxiety.
What are the risk factors for anxiety disorder?
Risk factors for anxiety disorder are listed below:
- Childhood abuse
- Experiencing or witnessing trauma
- Family history of anxiety disorders
- Shy or timid personality or personality prone to negative thinking
- Feeling distressed or nervous in new situations in childhood
- Stress buildup
- Having a medical condition or serious illness
- Personal history of other mental health disorders such as depression
- Drug or alcohol abuse
The abovementioned risk factors may increase susceptibility to anxiety disorders because they are associated with intense worry and stress. A person prone to anxiety may not be able to cope with these factors in a healthy manner, which may worsen their irrational thoughts and lead to a physical and psychological response in presence of triggers of their anxiety. For example, a medical condition or illness may increase the risk of anxiety disorders because a person may worry about issues such as treatment. Trauma is a risk factor because a person who witnessed or experienced it may not be able to find a way to cope with it.
Is anxiety disorder a severe mental condition?
Yes, anxiety disorder is a severe mental condition or serious mental illness. The definition of a serious mental illness is that it’s a mental, emotional, or behavioral disorder resulting in a serious functional impairment that significantly limits one or more life activities, according to the National Institute of Mental Health. Diagnostic criteria for anxiety disorders indicate the symptoms or disturbance impair the functioning of a patient. For that reason, anxiety disorder is a severe mental condition.
Is anxiety disorder genetic?
Yes, anxiety disorder is genetic i.e. it has a genetic component. According to a review by Sandra M. Meier of Dalhousie University in Canada and Jurgen Deckert of the University of Wurzburg from the March 2019 issue of Current Psychiatry Reports, anxiety disorders are moderately heritable, highly complex, and polygenic. That means multiple genes and genetic variations may play a role in the development of anxiety disorders.
Is anxiety disorder treatable?
Yes, anxiety disorder is treatable. The American Psychological Association explains that anxiety disorders are highly treatable; several months of psychotherapy can reduce or eliminate symptoms. In order to treat anxiety disorder, patients need to adhere to the treatment program. Support from family and friends is also beneficial.
