Is methocarbamol (Robaxin) addictive: abuse, side effects, and withdrawal



Methocarbamol abuse is the misuse of the muscle relaxant medication, often sold under the brand name Robaxin. Methocarbamol is a central nervous system (CNS) depressant with sedative and musculoskeletal relaxant properties. Excessive consumption and concomitant use with other substances leads to serious side effects.
The side effects of methocarbamol abuse are severe dizziness, facial swelling, confusion, poor coordination, blurred vision, slow heart rate, nausea or vomiting and seizures.
Methocarbamol causes withdrawal symptoms, but such reactions are generally mild and strong physical dependence is not usually viewed as a defining feature of Robaxin use. Under ordinary medical use, the drug is not widely known for causing a major withdrawal syndrome.
The symptoms of methocarbamol withdrawal include rebound muscle spasms or pain, anxiety, restlessness, sweating, headache, mood fluctuations, tremors and insomnia.
Is methocarbamol (Robaxin) addictive?
No, methocarbamol (Robaxin) is not considered physically addictive. However, misuse of the drug, such as taking excessive doses to achieve a sedative effect, potentially leads to psychological dependence.
Unlike other muscle relaxants or substances, methocarbamol does not typically cause cravings or withdrawal symptoms when use is discontinued. The drug’s sedative properties are relatively mild compared to other substances known for their addictive potential, such as opioids or benzodiazepines, making it a low-risk option for addiction.
Methocarbamol works by relaxing muscles and easing discomfort without inducing a strong sense of euphoria, reducing the likelihood of habitual misuse or it becoming habit-forming. Individuals increasing intake over time in search of a calming effect tend to experience dangerous outcomes.
The physical dependency risk remains low, but ongoing abuse fosters psychological reliance, prompting individuals to seek the drug despite adverse effects. To minimize risks, adhering to prescribed guidelines from healthcare providers ensures safe use and reduces misuse chances.
Can you get dependent on methocarbamol?

Yes, you can become dependent on methocarbamol. Dependence develops when the body starts relying on the drug for relief or relaxation, leading to repetitive use. Though methocarbamol does not trigger intense cravings, repeated consumption in higher amounts results in reliance.
Misuse results in a pattern of seeking temporary comfort, further reinforcing dependency. As psychological reliance builds, the drug becomes tied to stress relief. Even in the absence of physical withdrawal symptoms, quitting feels difficult when drug dependence sets in.
Is methocarbamol addictive at prescribed doses?
No, methocarbamol is not addictive at prescribed doses. The drug primarily serves as a muscle relaxant to address pain and stiffness, and when taken as directed, Robaxin doesn’t foster habits of misuse.
Methocarbamol does not trigger the compulsive behavior other drugs with stronger sedative effects cause. Most users are not likely to seek out methocarbamol once treatment ends, as the medication lacks the intense effects leading to excessive use.
Adhering to a doctor’s instructions helps maintain the drug’s effectiveness for the intended purpose, reducing the risk of misuse. When the prescribed dosage stays within recommended limits, methocarbamol does not promote dependence.
Users following the prescribed regimen are able to discontinue use without experiencing challenges. The medication provides effective relief for short-term muscle relaxation without fostering problematic use.
Are muscle relaxants addictive?
Yes, muscle relaxants have the potential for misuse and addiction, particularly with certain medications. Drugs like carisoprodol and diazepam are more prone to abuse due to their calming and sedative effects.
Both are classified as controlled substances, meaning they carry a higher risk of psychological dependence. Carisoprodol, often used for short-term muscle pain relief, leads to dependence if taken for extended periods or in larger amounts. Similarly, diazepam, a benzodiazepine, induces feelings of relaxation or euphoria when misused, heightening the risk of addiction.
A 2014 study by Witenko et al., titled “Considerations for the Appropriate Use of Skeletal Muscle Relaxants for the Management Of Acute Low Back Pain” revealed drugs such as carisoprodol and cyclobenzaprine are prescribed despite limited evidence supporting long-term effectiveness. Carisoprodol, in particular, carries a known abuse risk, prompting its reclassification as a controlled substance in 2012.
Muscle relaxants are commonly overused as well, with various patients exceeding the recommended duration. The potential for abuse and dependency, especially with carisoprodol, highlights the need for careful monitoring.
A 2020 paper by Mayank Gupta titled “Carisoprodol Abuse in Adolescence” described the case of a 16-year-old girl who began using carisoprodol to manage anxiety following personal losses and family issues, quickly increasing usage and experiencing withdrawal symptoms when attempting to quit.
The case highlighted growing concerns over carisoprodol abuse in adolescents. Despite this, carisoprodol misuse remains a significant public health issue due to its accessibility and addictive nature. Research shows combining carisoprodol with other substances produces effects similar to heroin.
Finally, according to a continuing education activity called “Diazepam,” last updated in August 2023 by Dhaliwal et al., diazepam is a Schedule IV controlled substance and has abuse potential.
Dependence and tolerance are likely to develop in individuals on long-term treatment or high doses, requiring careful supervision. Once dependence occurs, the odds of experiencing withdrawal symptoms increase.
What is methocarbamol abuse?
Methocarbamol abuse means using the medication outside medical direction for reasons unrelated to proper treatment. Abuse includes extra tablets, closely spaced doses or use of someone else’s prescription.
Methocarbamol acts as a central nervous system (CNS) depressant, so abuse usually involves pursuit of heavy drowsiness or sedation. Misuse shifts the drug from a short-term muscle-pain treatment into a substance used for altered awareness.
Danger rises sharply alongside alcohol, sleep medicines or opioid pain drugs because combined depression of brain activity becomes more severe. In practical terms, methocarbamol abuse is less about treatment and more about using Robaxin for a drug effect.
How common is methocarbamol abuse?
Recent official datasets do not provide a distinct prevalence figure for methocarbamol-specific abuse. According to a continuing education activity called “Methocarbamol” last updated in September 2024 by Sibrack et al., in the United States, methocarbamol accounts for more than 3 million prescriptions each year.
Animal research suggested lower abuse liability than barbiturates and benzodiazepines, yet human research still identified misuse potential. A separate NCBI review cited in the paper summarizing National Poison Data System data recorded 2,605 single-agent exposures from 2010 through 2020 among patients ages 6 to 19 involving carisoprodol, meprobamate, methocarbamol or metaxalone. Of those exposures, 75.74% were intentional.
Who is most at risk of misusing methocarbamol?
People with a past pattern of substance misuse, particularly involving sedatives, are most at risk of misusing methocarbamol. Risk increases among people already using alcohol, opioids, benzodiazepines or sleep medicines because methocarbamol adds more slowing and drowsiness.
A person chasing calm and heavy sedation is more vulnerable than someone using the drug solely for short-term muscle pain. Easy access plays a major role, with leftover tablets, family prescriptions and long refill periods all raising danger.
People already abusing sedating drugs are especially likely to treat methocarbamol as part of a larger cycle of misuse instead of a single substance.
What are the signs of methocarbamol abuse?
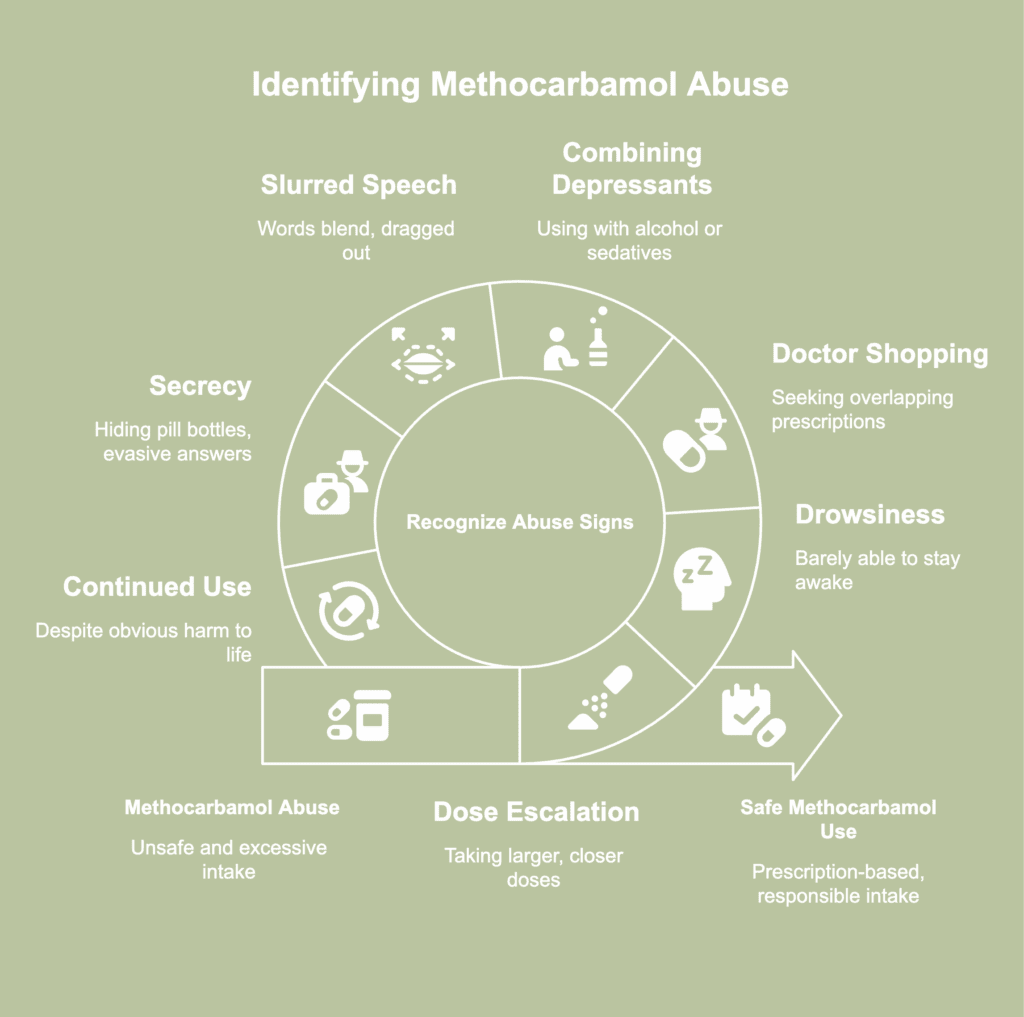
Signs of methocarbamol abuse refer to indications of unsafe and excessive methocarbamol intake. The signs of methocarbamol abuse are listed below.
- Dose escalation: A clear warning sign appears once a person starts taking larger amounts than the prescription permits or uses doses closer together for a stronger effect. Pill bottles empty sooner than expected, running out before the refill date arrives. Excuses about worsening discomfort start covering a growing drive to keep more of the medication in the body.
- Drowsiness: A person abusing methocarbamol appears barely able to stay awake, especially during hours normally allotted for work, school or daily responsibilities. Pronounced grogginess becomes visible through heavy eyelids, slowed reactions, poor balance and difficulty staying alert. Such presentation fits methocarbamol’s central nervous system depressant action.
- Doctor shopping: A recurring pattern of seeking overlapping prescriptions from several clinicians signals escalating misuse. Concern grows after repeated visits for the same complaint or claims about lost pills used to secure fresh supplies. According to a 2020 study by Soprano et al., titled “Assessment of Physician Prescribing of Muscle Relaxants in the United States, 2005-2016,” office visits involving either a new skeletal muscle relaxant (SMR) prescription like methocarbamol or ongoing SMR therapy rose from 15.5 million in 2005 to 30.7 million in 2016. New prescribing stayed largely unchanged, while continued SMR use tripled from 8.5 million to 24.7 million visits, indicating growth centered on long-term use rather than initiation. The study identified prolonged therapy, older adults and concurrent opioid use as the most concerning patterns in national prescribing.
- Using methocarbamol alongside alcohol or sedatives for a stronger effect: Misuse becomes evident if methocarbamol gets paired with alcohol, sleeping pills, opioids or similar depressants to deepen intoxication. Warning clues include timing pills around drinking sessions or speaking openly about chasing a heavier effect. Alertness falls faster, coordination worsens and judgment weakens once more than one depressant enters the system.
- Slurred speech: Words begin blending together, with syllables sounding dragged out or poorly formed during ordinary conversation. There’s delayed verbal delivery and sentences are ruined by muddled pronunciation. Telephone calls, casual chats and simple questions start revealing a voice pattern marked by poor clarity and weakened control.
- Secrecy around Robaxin use: Hidden pill bottles and evasive answers when asked about use signal an unhealthy relationship with Robaxin. A user starts shielding medication habits from family, inventing excuses about missing tablets or leaving rooms before taking another dose. Suspicion grows after frequent defensiveness and protectiveness surrounding bags, drawers or pockets. Concealment becomes a warning marker because honest medical use rarely requires persistent hiding.
- Continued use despite obvious harm: Use keeps going even after clear damage shows up in work, safety, health or close relationships. Missed work or a close call on the road fails to interrupt use for more than a brief stretch. Warnings from loved ones land with denial, irritation or a flat refusal to change course. Relentless use under worsening consequences marks a pattern driven by misuse and not just plain symptom relief.
What are the side effects of methocarbamol abuse?
Side effects of methocarbamol abuse describe an array of unwanted effects linked with methocarbamol use outside medical directions. The side effects of methocarbamol abuse are listed below.
- Severe dizziness: High-dose methocarbamol misuse dulls normal alertness and leaves the head feeling light. A quick rise from a chair makes vision and balance fall briefly out of sync. Walking across a room starts getting less steady even on level ground, and sudden turns are harder to manage with confidence.
- Facial swelling: Facial swelling occurs if methocarbamol triggers an allergic-type reaction, causing fluid to collect in soft tissue around the lips, cheeks or eyelids. Small blood vessels widen and leak fluid to nearby tissue, producing visible puffiness. Facial puffiness is likely to appear alongside hives, itching or breathing difficulty, especially after large doses or mixed-drug use.
- Confusion: Problematic use of Robaxin clouds thought and weakens the mind’s ability to organize information in a steady way. Conversation grows harder to follow and responses arrive late or miss the point. Familiar routines lose clarity without any obvious reason. Methocarbamol was one of the specific skeletal muscle relaxants (SMRs) evaluated in a 2013 study by Spence et al., “Risk of Injury Associated with Skeletal Muscle Relaxant Use in Older Adults.” The authors found an increased risk of injury with methocarbamol use, a finding presented alongside concern about confusion, sedation and related adverse effects in older patients.
- Poor coordination: Methocarbamol abuse disrupts precise motor control and makes movement less accurate. Hands begin missing small targets, while walking shows a subtle sway or delayed correction. Impaired coordination occurs as the drug suppresses central nervous system activity and weakens the smooth control needed for steady movement.
- Blurred vision: Visual clarity begins to fade, dulling visual sharpness and leaving objects looking hazy or unfocused. Reading becomes harder because letters seem smeared together, while faces and signs lose crisp edges. Eye changes create trouble judging distance, making ordinary movement seem less secure.
- Slow heart rate: A sluggish pulse develops and depresses normal body function. Weakness, unusual fatigue and faintness appear because blood circulation no longer keeps pace with normal demands. Standing up or walking across a room tends to be harder as heart activity drops below a healthy pace.
- Nausea or vomiting: Nausea or vomiting leaves someone unable to tolerate food or drink comfortably. Queasiness lingers in waves, then grows into retching or persistent vomiting after excessive intake. Physical strength drops further as fluid loss and stomach irritation begin draining energy.
- Seizures: Muscles stiffen without warning and jerking movements follow. Awareness subsequently disappears in the midst of an episode. Breathing problems and loss of consciousness create immediate danger for anyone entering such a state. A continuing education activity called “Methocarbamol” last updated in September 2024 by Sibrack et al., revealed drug monographs report seizures after IV administration in patients with epilepsy histories and in cases involving polysubstance toxicity. Product labeling notes neurologic adverse reactions occur more frequently, with sedation identified as the most common.
Does methocarbamol cause serotonin syndrome?
No, methocarbamol does not cause serotonin syndrome. Its drug profile centers on central nervous system depression and muscle relaxation, not serotonin elevation. Clinical concern around methocarbamol usually involves drowsiness, dizziness, slowed thinking and poor coordination.
A direct serotonin-driven mechanism does not sit within the usual clinical understanding of methocarbamol. Serotonin syndrome (SS) usually develops from medicines or drug combinations pushing serotonin signaling too high. Methocarbamol does not fit such a pattern on its own.
Risk becomes more relevant during combined use with certain antidepressants and migraine treatments, since such combinations raise the likelihood of serotonin syndrome. Under such circumstances, methocarbamol is not the main trigger.
Viewed plainly, methocarbamol alone is not a typical cause, but concurrent use with serotonin-affecting drugs raises a more serious concern.
Can you overdose on methocarbamol?
Yes, you can overdose on methocarbamol. An overdose happens after very high intake or after combining Robaxin with similar depressants like opioids, alcohol and benzodiazepines. Common warning signs include extreme drowsiness, vomiting, seizures and loss of consciousness.
A drug overdose is possible with misuse, unsafe mixing or long-term use that moves far beyond prescribed directions. Methocarbamol depresses CNS activity, and excessive amounts push normal brain and body function to a critical state.
Breathing becomes dangerously slow and collapse follows in severe cases. Emergency care is necessary if someone is unresponsive, has a seizure or shows major breathing problems after taking methocarbamol.
Can methocarbamol cause withdrawal symptoms?
Yes, methocarbamol can cause withdrawal symptoms. However, withdrawal linked with methocarbamol is generally not severe, and strong physical dependence is not usually regarded as a defining feature of Robaxin use.
In most cases, the drug is not known for producing a major withdrawal syndrome after ordinary medical use. The main concern tends to involve craving after misuse, especially if a person has grown attached to the calming or euphoric effect it produced.
Abrupt discontinuation after sustained high-dose consumption still leaves the body and mind unsettled for a period. Reactions are usually milder than withdrawal seen with more strongly dependence-forming substances.
Symptom intensity and duration of drug withdrawal differ according to the individual, the dosage taken and the length of use.
What are the symptoms of methocarbamol withdrawal?
Symptoms of methocarbamol withdrawal describe reactions emerging after methocarbamol use stops suddenly following prolonged usage. The symptoms of methocarbamol withdrawal are listed below.
- Rebound muscle spasms or pain: Cutting back on Robaxin sometimes causes muscles to be tighter and more reactive. Continual use dulls muscular tension for a period, then sudden reduction leaves the body struggling to regain balance without pharmaceutical suppression. Ordinary movement starts bringing sharper aching or renewed cramping because the relaxant effect no longer buffers baseline discomfort.
- Anxiety: An uneasy mental state develops after the familiar sedating effect is gone. Robaxin misuse creates a pattern in which calmness gets tied to persistent ingestion, and interruption leaves the nervous system unsettled. Thoughts begin moving faster, physical tension builds and minor stress is seemingly harder to absorb in early withdrawal.
- Restlessness: Inner agitation manifests as pacing or an inability to remain still for long. Quiet activities are harder to tolerate as comfort no longer comes easily. Restlessness marks a period of instability as the system adjusts after repeated exposure loses continuity. Sleep preparation turns frustrating because the body no longer eases into stillness as smoothly as before.
- Sweating: Temperature control and autonomic activity grow less steady during adjustment, leaving skin damp without physical exertion. Nighttime discomfort or sudden clamminess while resting makes the symptom particularly disruptive. Shirts get damp during sleep and sudden clamminess adds discomfort throughout the day.
- Headache: A pressing ache behind the eyes or across the forehead marks one withdrawal complaint linked with methocarbamol misuse. Quiet settings make the pounding feel harsher because attention has nowhere else to go. A bright screen or a short reading task quickly turns irritating under the pressure. Methocarbamol product labeling states neurologic adverse drug reactions occur more frequently, with sedation reported most often, followed by dizziness and headache, as noted in a publication authored by Sibrack et al., “Methocarbamol,” last updated in September 2024.
- Mood fluctuations: Emotional balance grows unstable, with irritation flaring without much warning. A small inconvenience draws a response stronger than the moment deserves. Minutes later, the edge subsides, yet the abrupt swing still disrupts ordinary conversation. Mood control wobbles for a period as the brain recalibrates without the drug.
- Tremors: Fine shaking of the hands marks another withdrawal complaint tied to methocarbamol misuse. Writing a short note or holding a cup demands extra concentration because the fingers no longer stay steady. An outside observer tends to notice just slight movements, yet routine tasks grow more difficult under constant trembling.
- Insomnia: Bedtime stretches to hours of wakefulness, with racing thoughts and repeated glances at the clock replacing normal rest. Continuous use had been supplying an artificial slowing effect, and abrupt removal strips away drug-driven sedation. Withdrawal then turns night into a draining pattern of broken rest, shallow sleep and exhaustion by morning.
What are the treatment options for methocarbamol abuse?

Treatment options for methocarbamol abuse refer to medical and supportive approaches used to address harmful and nonmedical methocarbamol utilization. The treatment options for methocarbamol abuse are listed below.
- Medical detoxification: Medical detoxification provides supervised care during early cessation. Clinicians monitor breathing, alertness and rebound symptoms while guiding a safer reduction plan. Close observation lowers the chance of sudden complications and helps manage discomfort without unsupervised self-treatment. According to a 2015 paper by Timko et al., titled “Patient and Program Factors that Bridge the Detoxification-Treatment Gap: A Structured Evidence Review,” detox completion and post-detox transition rates vary widely. As detox is not a stand-alone success, better outcomes depend on using detox as a bridge into continuing care, with motivational work, family involvement, peer support and active linkage to aftercare built into the program.
- Cognitive behavioral therapy (CBT): Cognitive behavioral therapy (CBT) targets thought patterns and daily routines feeding incessant drug use. Sessions help a person identify triggers, challenge false beliefs about relief or control and replace harmful habits with practical coping responses. Written exercises and guided reflection strengthen decision-making in cravings or stressful moments. Consistent CBT work supports stronger self-management and a lower likelihood of returning to misuse.
- Counseling: Counseling offers a private setting for discussing drug use, personal strain and barriers to recovery. Honest conversation with a trained professional helps uncover motives behind misuse and brings harmful patterns to clearer view. Individual guidance supports goal setting, relapse-prevention planning and healthier responses to pressure. Regular counseling often improves commitment to recovery by giving each stage of progress steady direction.
- Support groups: Shared discussion reduces isolation and gives practical insight from people who understand relapse pressure firsthand. Group accountability encourages honest check-ins and stronger follow-through outside meetings. Ongoing peer support helps recovery remain active in daily life instead of fading after formal treatment ends.
- Inpatient rehabilitation: Round-the-clock care gives a person distance from drug access and everyday pressures. Medical staff watch symptoms closely, manage complications and build a structured routine around recreation, meals and treatment sessions. Daily therapy inside a residential setting gives recovery stronger footing because outside distractions lose influence for a while. A longer stay strengthens discipline and readiness for life after discharge.
- Outpatient program: Various people need treatment while still keeping work, school or family responsibilities in place. An outpatient program offers scheduled therapy, recovery education and clinical oversight without requiring overnight residence. Appointments create accountability and keep progress moving while a person practices healthier decisions in ordinary surroundings. Real-world exposure gives clinicians a clearer picture of stressors, allowing coping strategies to match daily life more closely.
- Aftercare treatment: Recovery does not end once formal treatment concludes. Aftercare provides ongoing structure through follow-up counseling, relapse-prevention work and continued support after primary treatment finishes. Continued contact lowers the chance of drifting back to old habits, as warning signs receive attention before misuse takes hold again.
