Munchausen syndrome (factitious disorder imposed on self): definition, causes, symptoms, and treatments


Table of content
- What is Munchausen syndrome (factitious disorder imposed on self)?
- What are the causes of Munchausen syndrome (factitious disorder imposed on self)?
- What are the symptoms of Munchausen syndrome (factitious disorder imposed on self)?
- Who is affected by Munchausen syndrome (factitious disorder imposed on self)?
- What are the risk factors for Munchausen syndrome (factitious disorder imposed on self)?
- How is Munchausen syndrome (factitious disorder imposed on self) diagnosed?
- What are the treatments for Munchausen syndrome (factitious disorder imposed on self)?
- How to prevent Munchausen syndrome (factitious disorder imposed on self)?
- What to expect with Munchausen syndrome (factitious disorder imposed on self)?
- What is the difference between Munchausen syndrome (factitious disorder imposed on self) and Munchausen syndrome by proxy (factitious disorder imposed on another)?
- What is the difference between Munchausen syndrome (factitious disorder imposed on self) and malingering?
Munchausen syndrome, otherwise called factitious disorder imposed on self, is a mental health condition where a person intentionally fabricates or amplifies physical or psychological symptoms, often to gain medical attention or treatment.
The causes of Munchausen syndrome (factitious disorder imposed on self) include childhood trauma, personality disorders, desire for attention, frequent hospitalization and medical procedures, low self-esteem, and unmet emotional needs.
The symptoms of Munchausen syndrome are odd, vague, and inconsistent symptoms, frequent hospitalizations and medical interventions, self-infliction and aggravation, tampering with diagnostic tests and evidence, and reluctant to allow talking to family or previous healthcare providers.
Treatment options for Munchausen syndrome (factitious disorder imposed on self) include psychotherapy (talk therapy), cognitive behavioral therapy (CBT), family therapy, medication, and treatment of coexisting mental disorders.
What is Munchausen syndrome (factitious disorder imposed on self)?
Munchausen syndrome (factitious disorder imposed on self) is a mental illness where individuals repeatedly falsify physical or psychological signs and symptoms to appear ill, injured, or impaired. Deceptive behaviors involve fabricating medical histories, tampering with diagnostic tests, or self-inflicting harm to convince healthcare providers of an illness.
Motivation often stems from a deep-seated need for attention, sympathy, or validation rather than external rewards such as financial gain. Persistent engagement in such actions lead to unnecessary medical procedures, hospitalizations, and significant disruptions in daily life.
The term Munchausen syndrome was first coined by Richard Asher in 1951 and named after the 18th-century German aristocrat Karl Friedrich Hieronymus, Baron von Münchhausen, who enthralled audiences with incredible and dramatic tales of impossible feats, often featuring himself as the protagonist.
According to a publication last updated in July 2023, titled “Munchausen Syndrome” by Weber et al., inducing symptoms on purpose is not unusual; examples include willfully eating bad food, injecting insulin, picking at the skin, causing wounds, taking too much medication, and not taking prescription drugs as directed. Furthermore, patients have been known to alter test results and falsify medical records.
Why was Munchausen syndrome renamed to factitious disorder imposed on self (FDIS)?
Munchausen syndrome was renamed factitious disorder imposed on self (FDIS) to provide a more clinical and standardized terminology, removing associations with historical or non-medical references.
The previous name, derived from a literary figure known for exaggerated tales, was considered inappropriate for a serious psychiatric condition. Medical authorities advocated for a term accurately reflecting the disorder’s clinical nature without historical or fictional associations.
Another reason behind the name change was for the condition to align with the broader classification of factitious disorders in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5).
Renaming Munchausen syndrome as FDIS clarified its place within the category, emphasizing the self-imposed nature of symptom falsification. The updated term additionally improved diagnostic accuracy and consistency in medical and psychological settings.
Is Munchausen syndrome a mental illness?
Yes, Munchausen syndrome is a mental illness. FDIS is a rare and serious disorder classified under factitious disorders, characterized by the deliberate falsification or induction of physical or psychological symptoms.
Individuals with the disorder go to extreme lengths to appear ill, often undergoing unnecessary medical procedures or hospitalizations. Unlike malingering—a condition driven by fabricating illness for personal gain—FDIS stems from deep psychological distress and an intense need for attention or care. Proper diagnosis and treatment remain challenging due to the deceptive nature of the mental illness, making professional intervention essential.
How common is Munchausen syndrome?
Munchausen syndrome is considered rare, with fewer than 1% of patients in clinical settings receiving this diagnosis, according to a continuing education activity by Weber et al., titled “Munchausen Syndrome,” last updated in July 2023.
Due to the deceptive nature of the disorder, identifying true prevalence remains difficult, as a number of cases go undetected or are misdiagnosed. Individuals with the condition frequently change healthcare providers to avoid suspicion, making accurate tracking even more challenging.
The rarity of the diagnosis does not diminish its severity, since affected persons frequently require multiple medical operations, posing major health risks. Effective diagnosis and treatment of the disorder depend heavily on raised awareness and thorough assessment by medical specialists.
What are the causes of Munchausen syndrome (factitious disorder imposed on self)?
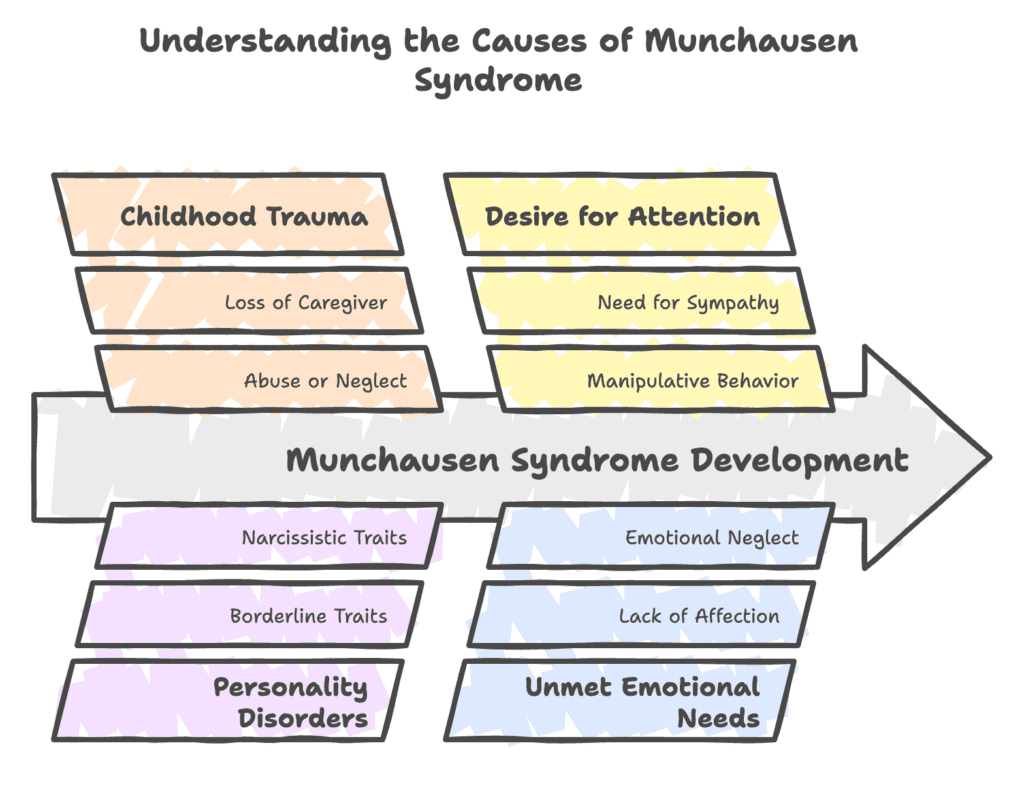
Causes of Munchausen syndrome (factitious disorder imposed on self) refer to underlying factors contributing to the development of the condition. The causes of Munchausen syndrome (factitious disorder imposed on self) are listed below.
- Childhood trauma
- Personality disorders
- Desire for attention
- Frequent hospitalization and medical procedures
- Low self-esteem
- Unmet emotional needs
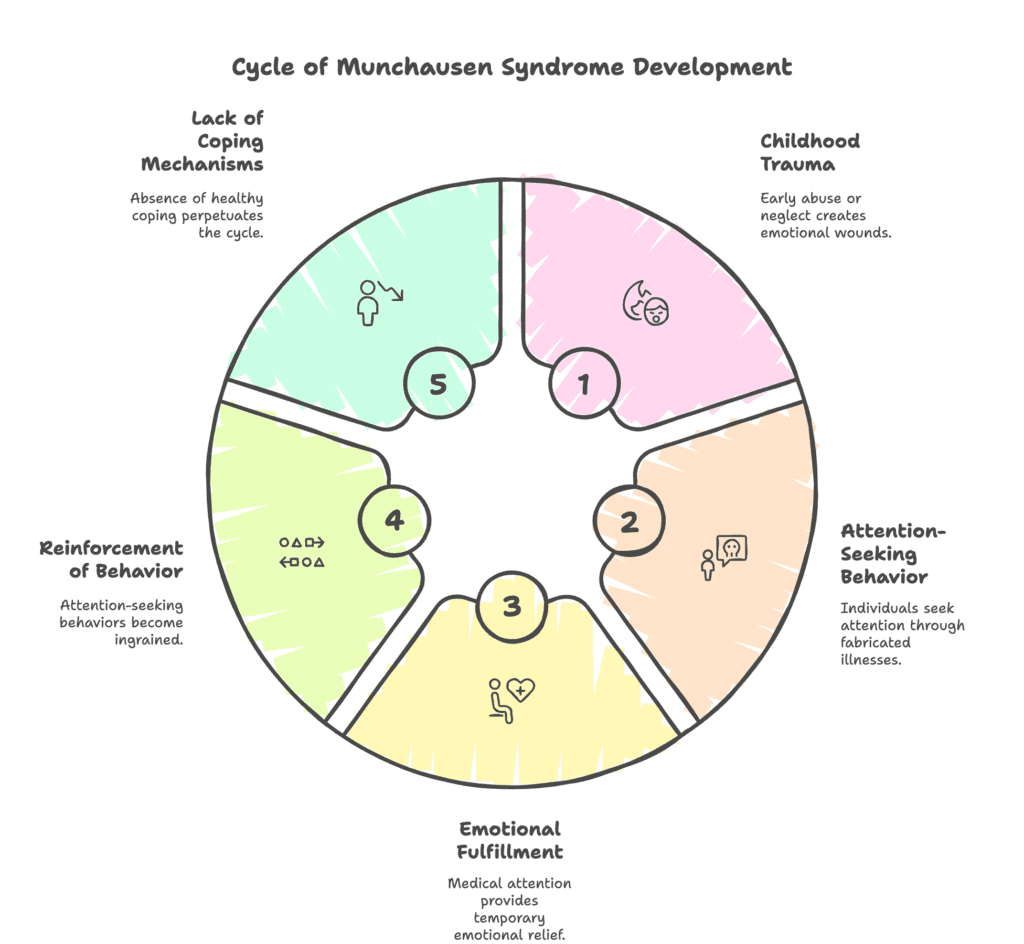
1. Childhood trauma
Childhood trauma contributes to Munchausen syndrome by creating deep emotional wounds manifesting through deceptive health-seeking behaviors. Abuse, neglect, or abandonment leads to feelings of worthlessness, insecurity, and an intense need for validation.
Seeking medical attention becomes a coping mechanism, as receiving care from healthcare providers provides comfort and a sense of importance. Early experiences of illness or hospitalization reinforce the idea of sickness bringing attention and emotional support.
Over time, fabricating symptoms becomes a learned behavior used to fulfill unmet emotional needs. Repeated deception about health additionally serves as a way to express unresolved pain without directly addressing traumatic memories.
As per an article by Kevin T. Carnahan and Anupam Jha, titled “Factitious Disorder” last updated in January 2023, the majority of experts concur that individuals with factitious disorders are significantly more likely to have experienced a challenging or traumatic upbringing.
Research analyzing conversations from factitious disorder online support groups revealed just three out of 57 participants reported having a positive upbringing. On the contrary, most reported experiencing different types of physical and mental abuse.
2. Personality disorders
Unstable emotions and distorted self-perception in personality disorders create a strong urge to seek attention through fabricated illness. A conscious effort to appear sick leads certain individuals to exaggerate symptoms or even cause self-inflicted injury.
Struggles in developing healthy connections create a strong desire for affirmation, making medical care a momentary source of comfort. When emotional impairment interferes with rational thought, lying about one’s health starts to feel like an essential coping strategy.
Others use manipulative tactics to keep control of their interactions with medical professionals, guaranteeing ongoing compassion and care. Intense fear of abandonment, common in certain personality disorders, fuels repeated hospital visits and unnecessary treatments.
3. Desire for attention
A strong need for attention drives individuals to fabricate illness, ensuring they remain the focus of care and concern. Medical treatment becomes a way to feel valued, especially when validation is lacking in other areas of life. Individuals consciously create or exaggerate symptoms, believing sickness guarantees sympathy and emotional support.
The desire to be nourished and prioritized causes frequent hospital visits and unneeded operations. A sense of control is gained by lying about one’s health, making it possible to manipulate social relationships in order to get ongoing attention.
Emotional distress often fuels such behaviors, making medical settings an appealing environment for readily available compassion.
4. Frequent hospitalization and medical procedures
Repeated hospital stays and medical procedures reinforce the belief that sickness leads to attention and care. The experience of undergoing treatment becomes familiar and even comforting, making the hospital feel like a secure place.
Individuals begin to associate personal worth with being a patient, leading to a cycle where fabricating illness feels necessary. The routine of medical visits and disease management fosters a sense of purpose, filling emotional voids left unaddressed.
Seeking treatment provides validation, especially when one feels neglected or insignificant. Anticipation of diagnosis or treatments becomes addicting, increasing reliance on medical intervention.
5. Low self-esteem
A lack of self-esteem pushes individuals to seek validation through illness, believing medical attention confirms personal significance. Pretending to be sick serves as a method to gain sympathy, offering temporary relief from deep-seated feelings of inadequacy.
Affected people often exaggerate symptoms to secure care and concern from doctors and loved ones. Producing false medical crises provides an escape from negative self-perceptions, redirecting attention from personal insecurities. The cycle of pretending to experience illness becomes deeply ingrained, as each instance of care reinforces the habit.
Without addressing underlying self-esteem issues, dependence on fabricated sickness persists, causing harm to the individual and the medical professionals involved in their medical care.
6. Unmet emotional needs
People with unfulfilled emotional needs are willing to conjure up illness in order to get treatment and validation. When personal relationships fail to give emotional support, people with FDIS have a need for attention and seek solace from healthcare professionals.
Getting treatment provides a fleeting sensation of significance, satisfying a strong need for connection. The behavior is strengthened by the contrast between the predictability of medical care and the unpredictable nature of personal relationships.
According to a 2024 paper by Nombora et al., titled “Munchausen Syndrome in the Context of Liaison Psychiatry: A Case Report and a Narrative Review,” the urge to play the “sick role” is one of the primary psychological drivers of factitious behavior, such as pretending to be ill or harming oneself.
The term describes the psychological and social advantages of being seen as sick, such as getting sympathy, care, and attention from others. The role offers constant support and emotional validation, filling a void individuals with Munchausen syndrome (MS) feel exists in their life.
What are the symptoms of Munchausen syndrome (factitious disorder imposed on self)?
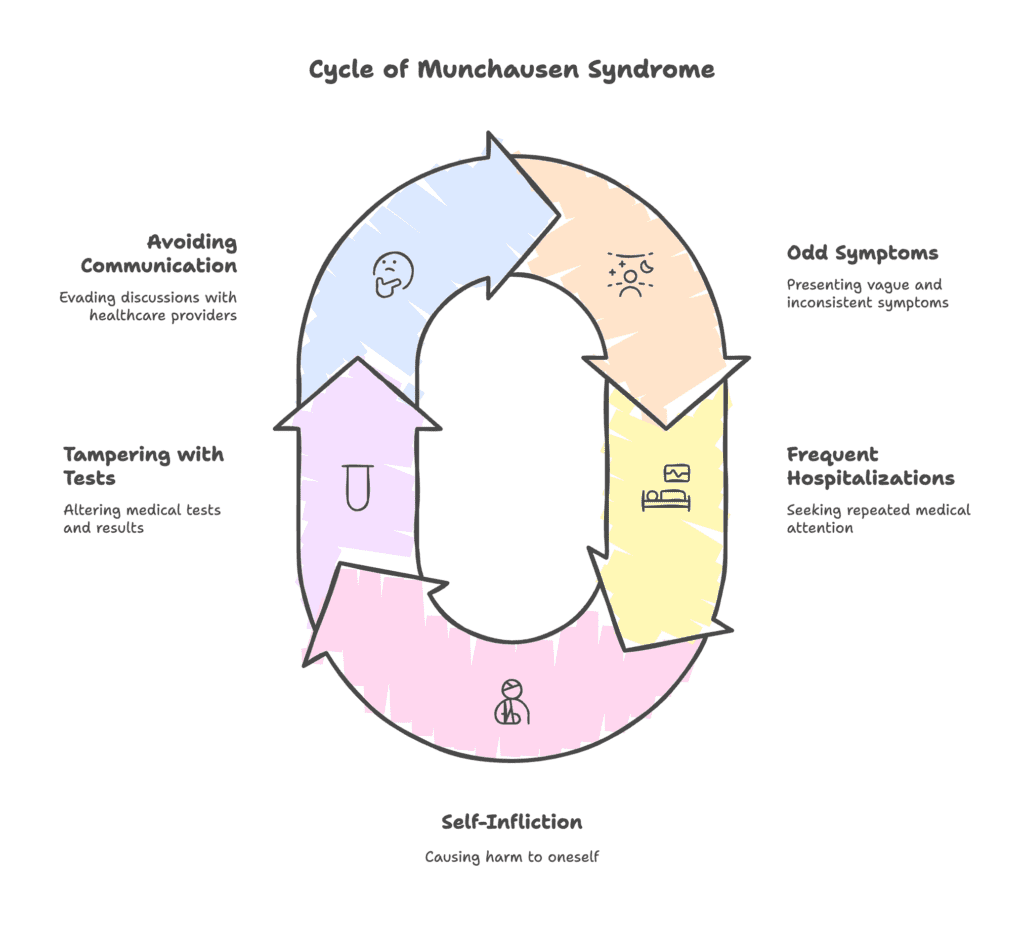
Symptoms of Munchausen syndrome (factitious disorder imposed on self) involve a pattern of persistent deception related to health. The symptoms of Munchausen syndrome (factitious disorder imposed on self) are listed below.
- Odd, vague, and inconsistent symptoms
- Frequent hospitalizations and medical interventions
- Self-infliction and aggravation
- Tampering with diagnostic tests and evidence
- Reluctance to allow talking to family or previous healthcare providers
1. Odd, vague, and inconsistent symptoms
Odd, vague, and inconsistent symptoms often signal Munchausen syndrome because individuals fabricate or induce illnesses rather than experiencing genuine medical conditions. Injecting toxic substances or tampering with wounds are examples of self-harming practices resulting in seemingly alarming symptoms, but do not correspond with established illness patterns.
Inconsistencies in medical history, test results, and reported experiences raise suspicion among healthcare providers, especially when symptoms seem to defy logical explanations. Individuals with FDIS offer elaborate details about health issues, yet descriptions frequently change or contradict earlier statements. Symptoms often intensify when under medical observation but suddenly improve once testing does not confirm an illness.
2. Frequent hospitalizations and medical interventions
Many hospitalizations and recurrent medical interventions often suggest Munchausen syndrome, since patients actively seek treatment despite not having a legitimate condition. Frequent visits to different healthcare facilities help avoid suspicion, allowing continued deception without detection.
Surgeries, diagnostic tests, and other invasive procedures become routine, driven by a deep need for medical attention and validation. Patients with FDIS run a high risk of iatrogenic injury.
A 2016 review article by Gregory P. Yates and Marc D. Feldman, titled “Factitious disorder: a systematic review of 455 cases in the professional literature” mentioned one patient featured in a 1997 study claiming to have undergone 42 surgical procedures during 850 admissions to 650 different institutions.
3. Self-infliction and aggravation
Individuals with MS often inflict injuries or aggravate existing conditions to maintain the appearance of illness. Self-inflicted wounds, tampering with medical devices, or ingesting harmful substances serve as methods to elicit concern from healthcare providers.
Acts of self-harm ensure symptoms appear severe enough to justify hospital visits and medical interventions. Certain patients aggravate minor ailments by interfering with the healing process, such as reopening cuts or infecting wounds, to prolong the need for treatment.
Self-inflicted illness or injury is present in 90% of factitious disorder (FD) cases, as noted in a 2020 article by Constanze Hausteiner-Wiehle and Sven Hungerer, titled “Factitious Disorders in Everyday Clinical Practice.”
Although intentional, self-infliction in FD is psychologically complex and frequently motivated by unconscious needs as opposed to external rewards. Patients’ actions worsen with time, raising medical risks.
4. Tampering with diagnostic tests and evidence
Tampering with diagnostic tests and medical evidence is a hallmark symptom of MS. Individuals with the factitious disease manipulate test results by contaminating samples, taking unprescribed medications, or falsifying medical histories to create the illusion of illness.
The complex nature of one’s dishonesty frequently results in lengthy and needless medical procedures, putting a great deal of stress on medical professionals. To keep the appearance of a chronic or worsening disease, patients falsify lab results or tamper with diagnostic procedures.
Detecting such falsifications is difficult for physicians because fake symptoms closely resemble actual ailments. The cycle of manipulation persists in the absence of appropriate psychological intervention, making diagnosis and therapy much more challenging.
5. Reluctance to allow care team to talk with family or previous healthcare providers
Reluctance to allow talking to family members or previous healthcare providers is a key symptom of Munchausen syndrome, often stemming from a desire to control the narrative surrounding their medical history.
Refusal to grant access to past records helps conceal inconsistencies in reported symptoms, preventing doctors from uncovering fabricated or self-induced illnesses. Individuals with FDIS fear exposure, knowing external input exposes a pattern of deception or unnecessary medical interventions.
Doctor shopping—the routine practice of seeking medical attention from several healthcare providers in an attempt to impede continuity of care—is one of the diagnostic problems in factitious disorder, as noted in a 2018 case report by Zeshan et al., titled “Challenges in Diagnosing Factitious Disorder.”
Patients routinely visit numerous emergency rooms at various locations, leading to needless imaging and laboratory tests, lengthier hospital stays, and resource overuse.
Who is affected by Munchausen syndrome (factitious disorder imposed on self)?
Munchausen syndrome typically affects women, the unmarried, and people working in the healthcare field. FDIS is additionally more common among individuals with borderline or histrionic personality features or disorders, as well as a history of sexual abuse, according to an article last updated in July 2023, titled “Munchausen Syndrome” by Weber et al.,
73.5% of FDIS patients in a 2021 research by Bérar et al., titled “A descriptive, retrospective case series of patients with factitious disorder imposed on self” were female, indicating FDIS is more prevalent in women.
Among patients with a known occupation, 47.1% had experience in healthcare. Nurses (9 cases), ambulance drivers, care assistants, life-support personnel, medical secretaries, and veterinary students were among the occupations.
What are the risk factors for Munchausen syndrome (factitious disorder imposed on self)?
Risk factors for Munchausen syndrome (factitious disorder imposed on self) refer to characteristics, experiences, or conditions increasing the likelihood of developing the condition. The risk factors for Munchausen syndrome (factitious disorder imposed on self) are listed below.
- Childhood trauma: Experiencing abuse, neglect, or abandonment during early years fosters deep emotional wounds, driving individuals to seek attention through fabricated illnesses. Emotional deprivation creates a lasting need for validation, making medical care a substitute for the nurturing absent in childhood. The association between receiving treatment and feeling valued becomes deeply ingrained, reinforcing deceptive health-seeking behaviors. Without healthy coping mechanisms, the cycle of feigned illness continues as a means of securing sympathy and reassurance.
- Frequent hospitalizations or chronic illness in the past: Individuals with a long history of medical treatments associate sickness with care, sympathy, and a sense of importance. The reinforcement of receiving attention during hospital stays creates a psychological link between illness and emotional fulfillment. The transition from genuine medical issues to fabricated symptoms becomes a way to maintain the familiar support system. The deep-rooted connection between past experiences and present behaviors makes unnecessary medical interventions feel justified.
- Exposure to illness in the family: Growing up in an environment focused on illness increases the likelihood of associating sickness with attention and care. Witnessing family members receive sympathy for medical conditions reinforces the idea of how being unwell results in special treatment. This learned behavior encourages individuals to replicate the dynamic, fabricating symptoms to elicit concern from others.
- Low self-esteem: Struggling with a poor self-image often leads individuals to fabricate illness as a means of feeling valued and significant. The notion of sickness being linked to worthiness of care drives repeated attempts to seek medical attention. Exaggerating symptoms provides an illusion of importance, offering temporary relief from feelings of inadequacy. The constant need for validation ensures the cycle of deception continues, reinforcing harmful behaviors over time.
- Extensive medical knowledge or healthcare background: People with a history of working in medical fields or frequent exposure to healthcare environments possess the expertise needed to fabricate convincing symptoms. Familiarity with medical terminology, diagnostic procedures, and treatment methods enables individuals to manipulate test results and deceive professionals more effectively. Medical knowledge not just facilitates deception but fosters a sense of control over interactions with doctors, reinforcing the compulsive behavior.
- A lack of meaningful relationships: Lacking social connections, individuals create illness as a way to gain attention and ensure constant acknowledgment. The structured environment of healthcare interactions offers reassurance, increasing dependence on fabricated sickness to address emotional emptiness. Without alternative sources of companionship, the cycle of medical deception persists, reinforcing the pattern of unnecessary interventions.
- Psychiatric disorders: Underlying mental health conditions, such as borderline personality disorder, depression, or anxiety, contribute to unstable emotions and a desperate need for validation. The emotional distress caused by such conditions increases the likelihood of engaging in self-harming behaviors to maintain the appearance of illness. Factitious disorder thrives in patients struggling with identity and emotional regulation, making psychiatric instability a significant risk factor.
How is Munchausen syndrome (factitious disorder imposed on self) diagnosed?
Munchausen syndrome (factitious disorder imposed on self) is diagnosed by doing a thorough evaluation focused on ruling out genuine medical conditions while assessing patterns of deception.
Physicians begin by conducting extensive tests, excluding legitimate illnesses before considering a psychological cause. Suspicious behavior, such as an unusual eagerness for medical procedures or inconsistencies in reported symptoms, raises concerns about intentional fabrication.
A defensive or evasive attitude when questioned about medical history further supports the possibility of a factitious disorder. Signs of made-up illnesses include symptoms not aligning with known disease patterns or improving when medical professionals are not present. Certain individuals go as far as presenting falsified test results or tampering with diagnostic samples to support claims.
The diagnosis is verified by medical professionals through psychiatric assessments, medical history reviews, and interviews. Since the condition is centered on deception, diagnosis is still difficult and frequently calls for cooperation from several specialists.
When does Munchausen syndrome occur?
Munchausen syndrome typically occurs during early-to-mid adolescence, with cases reported in girls as young as 9 years old, according to a 2005 review, titled “Factitious Disorder and Malingering in Adolescent Girls: Case Series and Literature Review” by Peebles et al.,
Patients aged 9, 10, 14, and 15 were diagnosed with factitious illness and frequently had self-inflicted wounds and complicated psychosocial histories. The case report proved factitious disorder is not limited to adults, contrary to previous assumptions.
What are the treatments for Munchausen syndrome (factitious disorder imposed on self)?
Treatments for Munchausen syndrome (factitious disorder imposed on self) refer to the therapeutic approaches and interventions designed to address the condition. The treatments for Munchausen syndrome (factitious disorder imposed on self) are listed below.
- Psychotherapy (talk therapy)
- Cognitive behavioral therapy (CBT)
- Family therapy
- Medication
- Treatment of coexisting mental disorders
1. Psychotherapy (talk therapy)
Psychotherapy (talk therapy) serves as the main treatment for Munchausen syndrome, helping individuals address the underlying psychological factors driving deceptive medical behaviors. Building self-esteem, enhancing emotional control, and lessening the need to fake or cause disease are the main goals of therapy sessions.
Building a strong therapeutic relationship is essential since various individuals with FDIS struggle to admit deceptive behaviors. Aside from encouraging healthier ways of addressing emotional needs without fabrication, ongoing counseling aids in identifying underlying reasons.
Sessions center on concurrent mental health issues, such as depression, anxiety, or unresolved trauma, that frequently have an impact on the illness. Consistent psychological support decreases harmful behavior and promotes authentic interactions with healthcare providers and loved ones. Successful treatment necessitates patience and commitment, as breaking the cycle of FDIS involves considerable work.
2. Cognitive behavioral therapy (CBT)
Cognitive behavioral therapy (CBT) targets the distorted thought processes leading individuals to fabricate or exaggerate medical conditions. CBT helps people understand why illness turns into a way to get approval by looking at the emotional causes leading to such actions.
Guided sessions focus on replacing lying with better coping mechanisms, thereby reducing the need to manipulate medical settings. Through structured exercises, individuals learn to recognize patterns of self-sabotage and develop alternative ways to fulfill emotional needs.
A 34-year-old woman with Munchausen syndrome was the subject of a 2011 study by Borojeni et al., titled “Münchausen’s Syndrome in the Form of Factitious Vomiting in a Young Female.” The patient purposefully caused vomiting in order to pretend to be ill.
Cognitive behavioral therapy, supportive psychotherapy, and sertraline (50 mg/day) were all part of the patient’s treatment regimen. Following treatment, she experienced fewer and less severe episodes of vomiting, and her mood considerably improved.
3. Family therapy
Family therapy is essential for resolving the relational factors contributing to MS. Therapy helps loved ones recognize enabling behaviors and set boundaries to prevent further reinforcement of falsified health concerns.
Honest conversations during a family therapy session help people understand the emotional challenges resulting in the fabrication of illnesses, reducing uncertainty and frustration across the family.
For the purpose of helping loved ones behave in ways promoting honesty rather than inadvertently validating harmful behaviors, family treatment focuses on teaching family members about factitious disorder.
Sessions allow for the restoration of trust, assisting both the individual and family members in navigating the disorder’s intricacies. Family members are assisted by therapists in promoting healthy coping strategies and diverting focus from illness-driven interactions.
4. Medication
No specific pharmacological treatment exists for Munchausen syndrome. Additionally, research concluded the disorder does not improve with antidepressants, antipsychotics, or other medical interventions, according to an article last updated in July 2023, titled “Munchausen Syndrome” by Weber et al.
Although most patients refuse, psychotherapy is the recommended treatment for all suspected Munchausen patients. The patient does not have to acknowledge having a factitious disorder, and most people rarely do. In certain instances, focusing cognitive-behavioral therapy on childhood trauma known to have caused the condition is beneficial.
5. Treatment of coexisting mental disorders
Addressing co-existing mental disorders helps reduce the emotional distress driving Munchausen syndrome. Treating depression lessens feelings of emptiness, decreasing the urge to fabricate illnesses for attention.
Managing anxiety lowers excessive health-related fears, making false reports of illness less appealing. Trauma therapy assists patients in processing past traumatic experiences, minimizing the desire to seek solace through feigned sickness.
Better emotional control and improved coping strategies are fostered by the proper treatment of personality disorders. Medication and counseling work together to stabilize mood, reducing the impulsive behaviors associated with FDIS.
Reliance on medical dishonesty diminishes when underlying illnesses improve, encouraging more truthful interactions. A comprehensive strategy focusing on mental health generally improves the likelihood of long-term recovery.
How to prevent Munchausen syndrome (factitious disorder imposed on self)?
There is no known way to completely prevent Munchausen syndrome. However, early intervention reduces the risk of severe complications. Recognizing warning signs, such as frequent unexplained illnesses or an intense preoccupation with medical care, allows for timely psychological support.
Addressing underlying suffering before negative patterns form is facilitated by promoting candid conversations about emotional difficulties. Building stronger social ties offers more healthful means of obtaining approval and attention.
Early therapeutic intervention is made possible by mental health assessments for people with a history of trauma or other psychiatric problems, helping identify persons at a greater risk. Raising awareness among families and healthcare providers about Munchausen syndrome improves recognition, allowing for early detection of concerning behaviors before escalation occurs.
While complete prevention remains uncertain, proactive mental health care and strong support systems lessen the chances of developing the condition.
What to expect with Munchausen syndrome (factitious disorder imposed on self)?
Living with Munchausen syndrome (factitious disorder imposed on self) involves repeatedly pretending to be ill, often going to extreme lengths to maintain the illusion. Individuals affected by the condition spend significant time trying to deceive medical professionals, making up symptoms or even physically hurting themselves to appear sick.
Convincing people of a major health problem turns into a constant endeavor resulting in repeated hospital stays, needless treatments, and a pattern of made-up medical emergencies. Constantly seeking medical care stresses relationships, undermines trust, and has long-term emotional and physical effects.
What are the complications of Munchausen syndrome?
Complications of Munchausen syndrome include infections, organ damage, overdose, physical harm, and emotional distress. Repeated medical interventions increase the risk of infections, especially when wounds are intentionally reopened or tampered with to maintain the appearance of illness.
Organ damage occurs due to unnecessary surgeries, prolonged medication use, or self-inflicted injuries weakening bodily functions over time. An overdose becomes a serious danger when medications are misused to trigger symptoms, leading to life-threatening consequences.
Physical harm results from self-inflicted injuries, excessive medical procedures, or repeated exposure to harmful substances. Emotional distress intensifies as deception becomes a way of life, creating feelings of guilt, anxiety, and isolation.
What is the difference between Munchausen syndrome (factitious disorder imposed on self) and Munchausen syndrome by proxy (factitious disorder imposed on another)?
The difference between Munchausen syndrome (factitious disorder imposed on self) and Munchausen syndrome by proxy (factitious disorder imposed on another) primarily lies in who is affected by the deceptive behavior. The difference between Munchausen syndrome (factitious disorder imposed on self) and Munchausen syndrome by proxy (factitious disorder imposed on another) are presented in the table below.
| Difference Between Munchausen Syndrome (Factitious Disorder Imposed on Self) and Munchausen Syndrome by Proxy (Factitious Disorder Imposed on Another) | ||
| Aspect | Munchausen syndrome (factitious disorder imposed on self) | Munchausen syndrome by proxy (factitious disorder imposed on another) |
| Definition | A psychiatric disorder involving fabrication, exaggeration, or self-induced medical conditions. | A disorder where a caregiver fabricates, exaggerates, or induces medical conditions in another person, usually a child or dependent. |
| Who is affected | The individual pretends to be ill or causes self-inflicted harm. | Another person, often a child or vulnerable individual, is made to appear sick or is harmed. |
| Motive | Seeks attention, sympathy, or validation through the role of a patient. | Gains attention and praise by appearing as a caring and devoted caregiver. |
| Deceptive behavior | Falsifies symptoms, manipulates test results, or deliberately injures oneself. | Creates or worsens another person’s symptoms by poisoning, suffocating, or tampering with medical care. |
| Medical consequences | Unnecessary medical tests, procedures, surgeries, and potential self-harm. | The victim suffers severe medical complications, long-term health damage, or even death. |
| Legal implications | Rarely leads to legal consequences unless insurance fraud or criminal acts occur. | Considered a form of abuse, leading to potential criminal charges and loss of custody. |
| Treatment focus | Psychological therapy to address underlying emotional issues and stop self-harm. | Intervention to protect the victim and psychological treatment for the perpetrator. |
Understanding the distinctions between Munchausen syndrome and Munchausen syndrome by proxy is crucial for recognizing warning signs and ensuring appropriate intervention. Although both are factitious disorders involving deceit and medical manipulation, the latter harms another person, therefore victim protection depends on early diagnosis.
What is the difference between Munchausen syndrome (factitious disorder imposed on self) and malingering?
The difference between Munchausen syndrome (factitious disorder imposed on self) and malingering mainly lies in motivation. The difference between Munchausen syndrome (factitious disorder imposed on self) and malingering are shown in the table below.
| Difference Between Munchausen Syndrome (Factitious Disorder Imposed on Self) and Malingering | ||
| Criteria | Munchausen syndrome (factitious disorder imposed on self) | Malingering |
| Motivation | Psychological need for attention and care | External rewards like financial gain, avoiding work, or obtaining medication |
| Awareness of deception | Aware of fabricating symptoms but not for material benefits | Fully aware and intentional, aiming for a specific goal |
| Behavioral patterns | Frequent hospital visits, tampering with medical tests, and self-inflicted harm | Exaggerating or inventing symptoms for personal gain while steering clear of medical tests designed to disprove claims. |
| Response to discovery | Often continues deception even when confronted | Stops faking symptoms once the goal is achieved or deception is exposed |
| Medical treatment | Seeks unnecessary medical procedures and interventions | Avoids treatment unless necessary for maintaining deception |
| Underlying cause | Driven by deep emotional distress, unresolved trauma, or a need for validation | Motivated by practical benefits, such as financial compensation or escaping responsibilities |
Both conditions involve deception related to illness, but Munchausen syndrome is rooted in psychological distress, while malingering serves a clear external purpose. Through addressing underlying psychological demands and avoiding needless medical treatments, a proper diagnosis ensures the right intervention.
