Dilaudid (hydromorphone) addiction: symptoms, effects, causes, and treatment



Dilaudid (hydromorphone) addiction is the uncontrollable use of the drug despite its negative effects. The condition is characterized by tolerance and withdrawal.
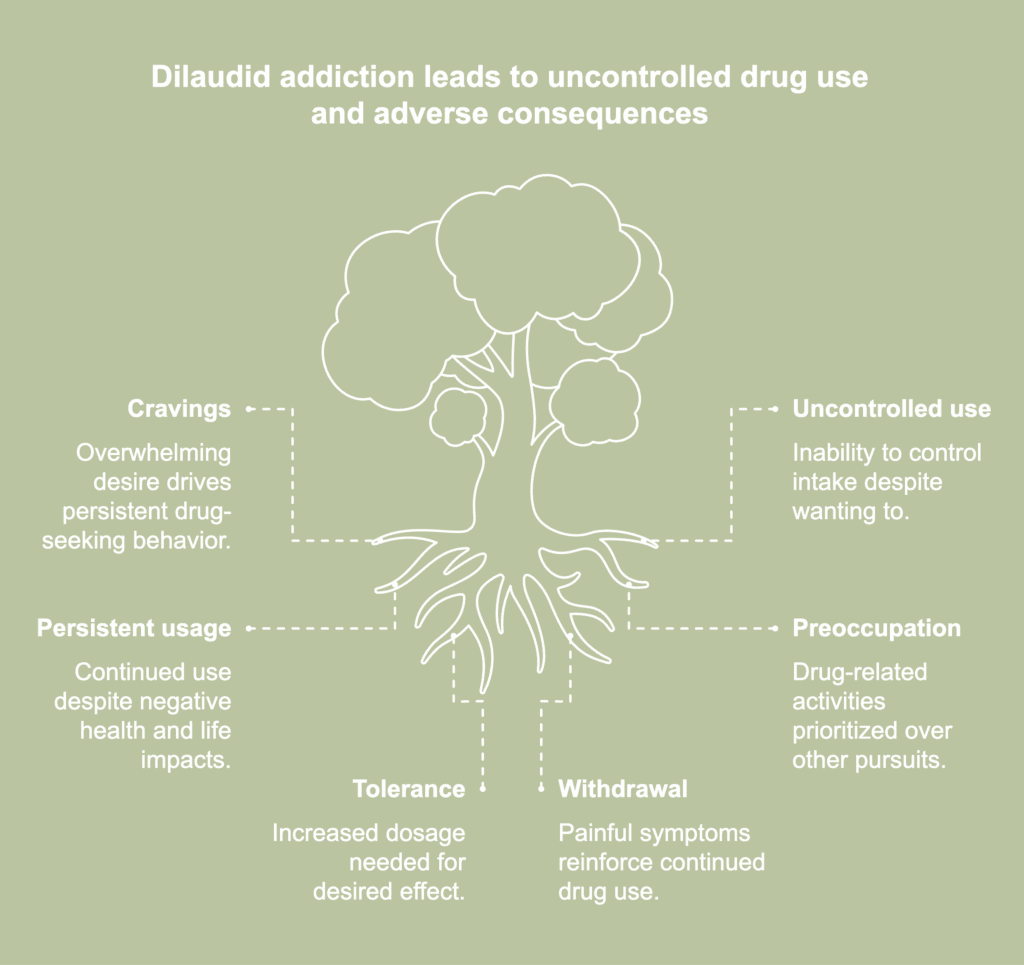
The symptoms of Dilaudid addiction are cravings for the drug, uncontrolled use, and persistent use despite its harms and/or in hazardous circumstances. Other symptoms include a preoccupation with drug-related activities, failure to fulfill personal and professional responsibilities, marked physical and cognitive changes, and the development of tolerance and withdrawal.
The effects of Dilaudid addiction are adrenal insufficiency, organ damage, urinary retention, cognitive impairment, an increased risk of overdose, suicidal ideations, and impaired quality of life.
The causes of Dilaudid addiction are misuse, self-medication, a dysregulated dopamine pathway, drug-induced hyperalgesia, and the development of tolerance, dependence, and withdrawal.
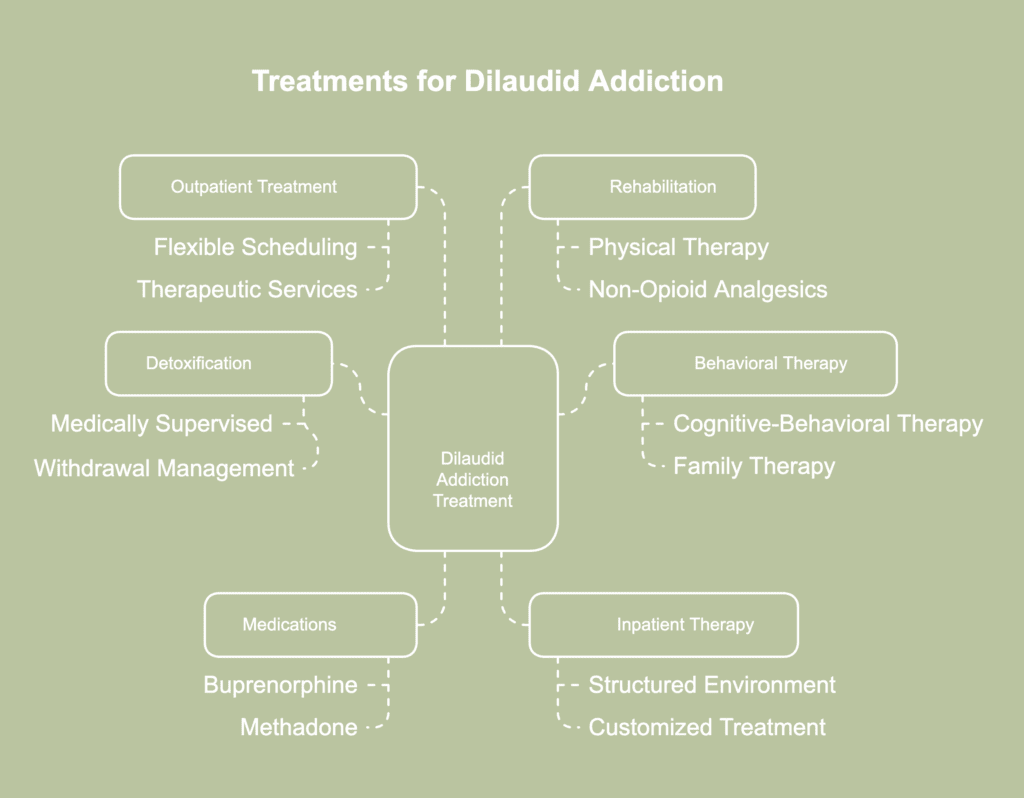
The treatments for Dilaudid addiction are detoxification, inpatient therapy, outpatient therapy, behavioral counseling, medications, and rehabilitation.
What is Dilaudid (hydromorphone) addiction?
Dilaudid (hydromorphone) addiction refers to a condition characterized by uncontrolled and compulsive use of the substance even when drug use leads to adverse outcomes. The condition is marked by physical dependence on the drug and the manifestation of cravings and withdrawal symptoms. An addiction to Dilaudid (hydromorphone), a semi-synthetic opioid, exhibits features similar to those that characterize a Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) diagnosis of opioid use disorder.
According to SAMHSA’s 2023 publication titled “Key Substance Use and Mental Health Indicators in the United States: Results from the 2022 National Survey on Drug Use and Health,” among individuals aged 12 years or older using prescription pain relievers in the previous year, 1.2% reported misusing hydromorphone. Among those who used prescription hydromorphone in the past year, 7.9% reported misusing it. The problem of Dilaudid (hydromorphone) addiction is a part of a larger crisis involving the abuse and misuse of prescription opioids.
What is Dilaudid (hydromorphone)?
Dilaudid (hydromorphone) is the brand name of hydromorphone, a semi-synthetic opioid with analgesic properties. Dilaudid is used for treating moderate to severe chronic pain and specific forms of cough. It is prescribed for a short duration in cases where alternative analgesics are not tolerated or fail to produce the desired effects. Its active ingredient is hydromorphone hydrochloride, and it is available in a tablet and liquid form for oral ingestion. Dilaudid is available only with a prescription that has been issued by a licensed medical practitioner.
How strong is hydromorphone compared to other opiates?
Hydromorphone is 2-8 times more strong as an analgesic agent compared to opiates like morphine, as stated by the United States Drug Enforcement Administration in their web publication titled “Hydromorphone.” Hydromorphone formulations like Dialudid have been found to be 5 times stronger than heroin on a milligram basis, according to a 1990 article by Wallenstein et al., published in the journal Pain, titled “Clinical analgesic assay of repeated and single doses of heroin and hydromorphone.”
What is the difference between Dilaudid and morphine?
The difference between Dilaudid and morphine stems from their nature, potency, effects, and safety profiles. The differences are described in the table below.
| Dilaudid | Morphine |
|---|---|
| Dilaudid is the brand name of the generic drug hydromorphone. | Morphine is a generic drug. |
| It is available in a tablet and liquid form for oral administration. | It is available as an immediate-release tablet, an extended-release tablet, an extended-release capsule, and as a syrup or a powder that is dissolved in water for oral administration. |
| Hydromorphone formulations like Dilaudid have a more rapid onset of action because they cross the blood-brain barrier quickly. | Morphine has a slower onset time. |
| As a hydromorphone formulation, Dilaudid is 2-8 times stronger than morphine. | Morphine is less strong than an equivalent dose of Dilaudid. |
| Its effects last for a shorter duration than those of morphine. | Its effects last longer than those of Dilaudid. |
| It has a shorter half-life compared to morphine. | It has a longer half-life. |
| Dilaudid’s sedative action is more potent than that of morphine. | Morphine’s sedative property is weaker. |
| It produces greater euphoric effects compared to morphine. | It produces less euphoria than hydromorphone formulations. |
| Hydromorphone formulations like Dilaudid provide superior pain management than morphine in cases of acute pain. | Morphine is less effective for acute pain. |
| Hydromorphone formulations like Dilaudid are safer for individuals with renal insufficiency. | Morphine is considered less safe for individuals with impaired renal function. |
| Side effects like nausea and vomiting are reported less when hydromorphone formulations like Dilaudid are used. | More instances of side effects like nausea and vomiting have been noted compared to hydromorphone. |
| Fewer instances of constipation are recorded in a section of users. | More instances of side effects like constipation were recorded. |
| Fewer pre-, peri-, and post-operative patients have reported side effects like itching. | More individuals in the same population have reported itching. |
| Fewer events of respiratory depression have been noted in populations undergoing orthopedic surgical procedures. | More instances of respiratory depression were noted in the same population. |
| Fewer instances of urinary retention have been recorded in individuals undergoing an orthopedic surgical procedure. | There were more occurrences of urinary retention in this population. |
| Compared to morphine, rescue drugs have been used in more instances in patients treated with hydromorphone in medical and surgical settings. | Rescue drugs have been used in fewer instances in patients treated with morphine. |
| The average length of stay (LOS) in the hospital is shorter for patients treated with hydromorphone. | On average, the LOS is longer for patients treated with morphine. |
| The 30-day hospital readmission rate for any cause is higher among patients treated with hydromorphone. | The 30-day all-cause hospital readmission rate is lower for patients treated with morphine. |
| At present, there is a shift toward using hydromorphone formulations like Dilaudid as a first-line analgesic agent. | The use of morphine in medical and surgical cases has decreased in recent times. |
| Dilaudid tends to be more expensive than morphine because the former is a brand-name product. | Morphine is less expensive because it is a generic drug. |
What makes Dilaudid addictive?
The ability to induce tolerance and physical and/or psychological dependence makes Dilaudid addictive. The addictive potential of Dilaudid is explained by how opioids in general affect the brain and trigger addiction.
Hydromorphone, the active ingredient in Dilaudid, is a powerful opioid that binds to mu-opioid receptors in the brain. With continuing use, the cells containing the opioid receptors become less responsive to the effects of the opioid. So, the individual needs to take more of the drug to derive the same effect. Thus, tolerance develops. Individuals who take hydromorphone are known to develop tolerance to the drug even at therapeutic doses and with short-term use. With increasing dosage, brain functionality is altered. The brain, accustomed to the presence of drugs, begins to malfunction in their absence. Thus, dependence develops. The individual experiences unpleasant physical effects when they are not taking drugs. This is withdrawal syndrome, which is triggered by tolerance. Individuals feel compelled to continue using the drug to escape the discomfort of withdrawal.
The ability of Dilaudid to produce euphoria contributes to its addictive potential. Besides being present in the neural areas linked to the perception of pain, mu-opioid receptors are also concentrated in the reward regions of the brain. This explains why opioid medications like Dilaudid produce euphoria. The rewarding effects of opioids are magnified the quicker the drug reaches the brain. Hydromorphone formulations like Dilaudid have a rapid onset of action because they are able to permeate the blood-brain barrier quickly. The Food and Drug Administration (FDA) notes in its drug fact sheet titled “ “DILAUDID ORAL LIQUID AND DILAUDID TABLETS (hydromorphone hydrochloride): CS-II” that peak plasma hydromorphone level is reached within a mere ½-1 hour of ingesting 8 mg Dilaudid. The user gets an immediate “high,” which explains the appeal of the drug among recreational users. It is possible for individuals who have been taking Dilaudid to manage pain to feel the urge to take the drug repeatedly to experience its high.
How addictive is Dilaudid?
Dilaudid is highly addictive, and its active ingredient hydromorphone has been classified as a Schedule II controlled substance by the Drug Enforcement Administration (DEA). A DEA Schedule II substance has a high abuse potential and an increased risk of triggering physical and psychological dependence. Although Dilaudid is highly addictive, there is no evidence to suggest that hydromorphone has more abuse potential than materially similar drugs, such as morphine and other pure opioid agonists, according to a 2005 article by Alison Murray and Neil A. Hagen published in the Journal of Pain and Symptom Management, titled “Hydromorphone.”
What are the symptoms of Dilaudid addiction?
The symptoms of Dilaudid addiction are listed below.
- Cravings: Craving is defined as a powerful and overwhelming desire to use a drug. It is a core feature of all substance use disorders. It is triggered by drug-related cues in the environment, mental stress, and unpleasant withdrawal symptoms.
- Uncontrolled drug use: Individuals who are addicted to Dilaudid find themselves unable to control how much of the drug they take, despite wanting to. They tend to take more than the amount prescribed by their physician or more frequently. Individuals with addiction are known to resort to “doctor shopping,” the practice of seeing multiple treatment providers to obtain multiple prescriptions, to acquire the drugs. Compulsive and uncontrolled drug use is a hallmark of addiction and results in the inability to quit despite wanting to.
- Persist usage despite adverse consequences: Individuals addicted to Dilaudid continue using the drug despite experiencing its negative effects. These adverse effects include negative health outcomes, dysfunctional interpersonal relationships, inability to fulfill professional obligations, financial hardship stemming from job loss or increasing expenses incurred to purchase the drugs, and legal troubles.
- Increased preoccupation with drug-related activities: As their addiction problem intensifies, individuals spend increasing amounts of time thinking about using the drug, procuring the substance, consuming it, and recovering from its effects. They prioritize these drug-related activities over meaningful social, occupational, and recreational pursuits.
- Failure to fulfill responsibilities: Individuals with Dilaudid addiction fail or are unable to fulfill their personal and professional responsibilities because they are either preoccupied with drug-related activities or have been rendered incapable due to drug-induced physical and/or psychological impairments.
- Drug use in hazardous situations: Individuals with Dilaudid addiction have been observed to use the substance in physically hazardous circumstances, such as driving a vehicle or operating heavy machinery when intoxicated.
- Development of tolerance: Long-term use of Dilaudid induces tolerance in a section of users. They need the drug more frequently or in increasing amounts to derive the earlier or the desired effect.It has been observed that tolerance to the analgesic and euphoric effects of opioids develops rapidly, according to a 2016 article by Volkow et al., published in The New England Journal of Medicine, titled “Opioid Abuse in Chronic Pain — Misconceptions and Mitigation Strategies.”
- Manifestation of withdrawal symptoms: Experiencing withdrawal symptoms after quitting Dilaudid is an indication that the individual has developed dependence on the drug. Painful and uncomfortable withdrawal symptoms contribute to the maintenance of addiction.
- Physical changes: Physical signs like constricted pupils, unexplained drowsiness, and slurred speech are abnormal and should be considered as red flags in individuals known to be using Dilaudid. These signs indicate that the individual is misusing the drug or has become addicted to it.
- Cognitive impairments: The onset of cognitive problems like reduced attention, impaired memory, and faulty decision-making indicates that an individual taking Dilaudid is misusing it or has possibly developed an addiction to it.
What are the effects of Dilaudid addiction?
The effects of Dilaudid addiction are listed below.
- Adrenal insufficiency : Long-term opioid use in high doses, a practice prevalent among individuals with chronic pain, inhibits the hypothalamic-pituitary-adrenal (HPA) axis, possibly causing serious adrenal insufficiency. The condition manifests as a cluster of non-specific symptoms like fatigue; lack of appetite; gastrointestinal issues like diarrhea, nausea, and vomiting; orthostatic hypotension; musculoskeletal pain; sexual dysfunctionality; and mood changes.
- Organ damage: It is possible for Dilaudid addiction to damage organs like the liver, kidneys, and brain.
- Urinary retention: Opioid pain medications impair the movement of gut muscles. Thus, it is harder for the bladder muscles to function properly, resulting in urinary retention.
- Cognitive impairment: Long-term prescription opioid use has been linked to mild cognitive impairment in older adults, according to a2022 article by Warner et al., published in the Journal of the American Geriatric Society, titled “Prescription Opioids and Longitudinal Changes in Cognitive Function in Older Adults: A Population-Based Observational Study.” Among all cognitive domains, the maximum adverse drug impact on the brain in this population has been observed for memory.
- Suicidal ideations: Addiction to pain medications is a risk factor for developing suicidal thoughts and behaviors like planning and attempting, according to a 2024 article by Giugovaz et al., published in the journal Psychiatry Research, titled “Substance addictions and suicidal thoughts and behaviors: Evidence from a multi-wave epidemiological study.”
- Increased risk of overdosing : Compulsive and uncontrolled drug use is a hallmark of addiction. This behavior increases the risk of an individual overdosing. The risk of an overdose magnifies if Dilaudid is mixed with alcohol and other opioids. Abusing Dilaudid by chewing, crushing, snorting the powdered drug, or injecting the dissolved substance increases the risk of overdosing. It is possible for overdosing to cause severe respiratory depression that results in coma and death.
- Impaired neonatal health: Infants born to mothers addicted to Dilaudid exhibit neonatal withdrawal syndrome characterized by respiratory depression and withdrawal symptoms.
- Impaired quality of life: Substance abuse causes negative physical health outcomes, strains interpersonal relationships, and impairs an individual’s ability to function effectively at their workplace or in school by causing cognitive deficits. Poor workplace performance and/or increased spending on the substance of abuse cause financial hardships that affect not only the individual but also their families. There is an increased risk of the individual becoming involved in illegal activities like drug trafficking that invite legal penalties.
- Withdrawal syndrome: Physical and/or psychological dependence on Dilaudid causes unpleasant withdrawal symptoms when the drug is stopped abruptly.
What are the causes of Dilaudid addiction?
The causes of Dilaudid addiction are listed below.
- Misuse: Therapeutic opioid misuse is alarmingly prevalent.The National Institute on Drug Abuse in their June 2021 release titled “Prescription Opioids: DrugFacts” notes that individuals tend to misuse prescription opioids by taking the drug in a way that has not been prescribed, such as taking it in excessive doses or more frequently, or using it recreationally to derive a “high.” A significant percentage of individuals obtain these drugs from family members and friends or engage in “doctor shopping.”
- Self-medication: There is robust scientific evidence to suggest that individuals who use opioids frequently, such as those who have been prescribed such drugs, tend to self-medicate negative emotional states with opioids.
- Dysregulation of the dopamine pathway: Dysregulation of the dopamine pathway is caused by both chronic pain and chronic opioid use. Neuroinflammation triggered by chronic pain and opioid use causes dysphoria. It is a state that produces negative emotions, such as anxiety and depression, by dysregulating the mesocorticolimbic dopaminergic pathway implicated in reward salience and motivated reward-seeking behaviors. Long-term opioid use magnifies the negative emotions associated with chronic pain. It is possible for individuals taking opioid analgesics for managing pain to become dependent on the euphoric effects of the drugs to soothe their negative emotions. On the other hand, prescription opioids are independently reinforcing through their analgesic effects, according to a 2016 article by Taylor et al., published in the journal Pain, titled “Mesolimbic dopamine signaling in acute and chronic pain implications for motivation, analgesia, and addiction.” Opioid analgesics directly dampen pain pathways via their action on the central and peripheral nervous systems. These analgesic effects are perceived as rewards by the individual. Simultaneously, the stimulation of the dopamine pathway by the opioids drives reward-seeking behaviors, characterized by repeated drug-use attempts.
- Development of hyperalgesia: In a section of users taking opioid pain medications, it has been observed that repeated administration induces hyperalgesia, a state marked by increased sensitivity to pain, according to 2016 article by Volkow et al., published in The New England Journal of Medicine, titled “Opioid Abuse in Chronic Pain — Misconceptions and Mitigation Strategies.” Hyperalgesia compels individuals to increase drug dosage inappropriately, which raises their risk of developing tolerance.
- Development of tolerance: Long-term use of opioids for their analgesic properties triggers the development of tolerance (Volkow et al., 2016). The individual requires increasingly higher doses of the drug to derive the same analgesic effect. Tolerance to the euphoric effects of analgesic opioids, too, develops rapidly and causes individuals to increase dosage.
- Development of dependence: The increased use of opioid analgesics tends to exacerbate pain instead of alleviating it (Volkow et al., 2016). A vicious cycle thus develops that eventually triggers the addiction problem by making the individual dependent on the drug. On the other hand, tolerance to the euphoric effects of opioid analgesics increases the likelihood of the drug-taking individual developing psychological dependence on the drug. Psychological dependence on opioid analgesics is likely in individuals who self-medicate their symptoms of mental stress, anxiety, and/or mood disorders with these drugs. The development of dependence is one of the most potent causes of addiction.
- Development of withdrawal syndrome: The development of dependence on prescription opioids is marked by neural adaptations. Drug-induced changes in the brain cause unpleasant withdrawal symptoms to manifest when drug use is stopped. Compulsive drug-taking behaviors are often the result of an individual trying to escape the pain of withdrawal.
What are the treatments for Dilaudid addiction?
The treatments for Dilaudid addiction are listed below.
- Detoxification: Undergoing a medically supervised drug detoxification process makes the withdrawal process safe and comfortable. The patient remains stable as the drug is gradually eliminated from the body. A medically-supervised detox is typically carried out at an inpatient addiction treatment facility where the patient is monitored 24×7 by a professional healthcare team. Depending on the severity of the addiction problem and how withdrawal progresses, patients are prescribed medications to treat the addiction disorder and/or ease withdrawal symptoms. Individuals with severe Dilaudid addiction are gradually weaned off the drug. Depending on the duration and severity of their addiction problem, it is safe for patients to undergo drug detoxification at an outpatient facility with limited medical monitoring.
- Behavioral therapy: Behavioral therapies for addiction seek to modify a patient’s attitudes, behaviors, and expectations associated with drug use, improve life skills, and spur motivation to seek and/or continue therapy. Cognitive-behavioral therapy (CBT) aims to help patients identify maladaptive thoughts, emotions, and behavioral responses that contribute to their addiction problem and replace these with positive and pro-abstinence ones. Multidimensional family therapy, designed for adolescent drug users, aims to improve a patient’s functioning in multiple areas of life by addressing personal and family factors that contribute to their drug-use behaviors, according to a June 2021 National Institute on Drug Abuse (NIDA) release titled “Prescription Opioids: DrugFacts.” Contingency management is a recognized tool for treating drug abuse. Behavioral therapies are delivered in individual, group, and family counseling sessions.
- Medications: The FDA has approved the use of buprenorphine and buprenorphine formulations like Suboxone (a combination of buprenorphine and naloxone), methadone, and naltrexone for the treatment of opioid addiction. Buprenorphine/naloxone formulations and methadone have been found to reduce cravings in individuals with prescription opioid use disorder, according to a 2022 article by McAnulty et al., published in the journal Drug and Alcohol Dependence, titled “Buprenorphine/naloxone and methadone effectiveness for reducing craving in individuals with prescription opioid use disorder: Exploratory results from an open-label, pragmatic randomized controlled trial.” Medications are used as part of an opioid replacement, maintenance, or substitution therapy. This involves using an opioid with less addictive potential and a greater safety margin than the problematic opioid. Medications like clonidine are prescribed as adjunct therapy to ease withdrawal symptoms while the methadone or buprenorphine dosage is being modified. Clonidine reduces symptoms like high blood pressure, elevated heart rate, insomnia, and anxiety. Over-the-counter drugs are used to ease uncomfortable withdrawal symptoms like nausea, vomiting, and diarrhea.
- Inpatient therapy: Inpatient addiction treatment facilities provide intensive 24×7 medical care and monitoring of the patient at a residential facility in a structured and drug-free environment. The treatment regimen is customized to suit the unique needs, addiction severity, and medical condition of a patient. The patient is required to stay at the facility throughout the length of the treatment.
- Outpatient treatment: Outpatient addiction recovery facilities allow individuals with Dilaudid addiction to access treatment services without needing to stay at the facility. They continue working, attend school, and fulfill personal responsibilities while undergoing treatment. Outpatient treatment facilities provide care at varying levels of intensity via multiple therapeutic services in different formats, depending on the needs and daily schedules of the patient.
- Rehabilitation: As Dilaudid is a powerful and effective pain medication, an intervention to treat an addiction to the drug should include strategies for long-term pain management that do not involve relying on opioid pain medications. Physical therapy, use of non-opioid analgesics, and patient education about managing pain symptoms are effective rehabilitation measures to promote sustainable addiction recovery. Other effective pain management strategies include enhancing physical fitness, improving general health, pacing activities, learning and practicing relaxation techniques, and engaging in meaningful social interactions.
What are the symptoms of Dilaudid withdrawal?
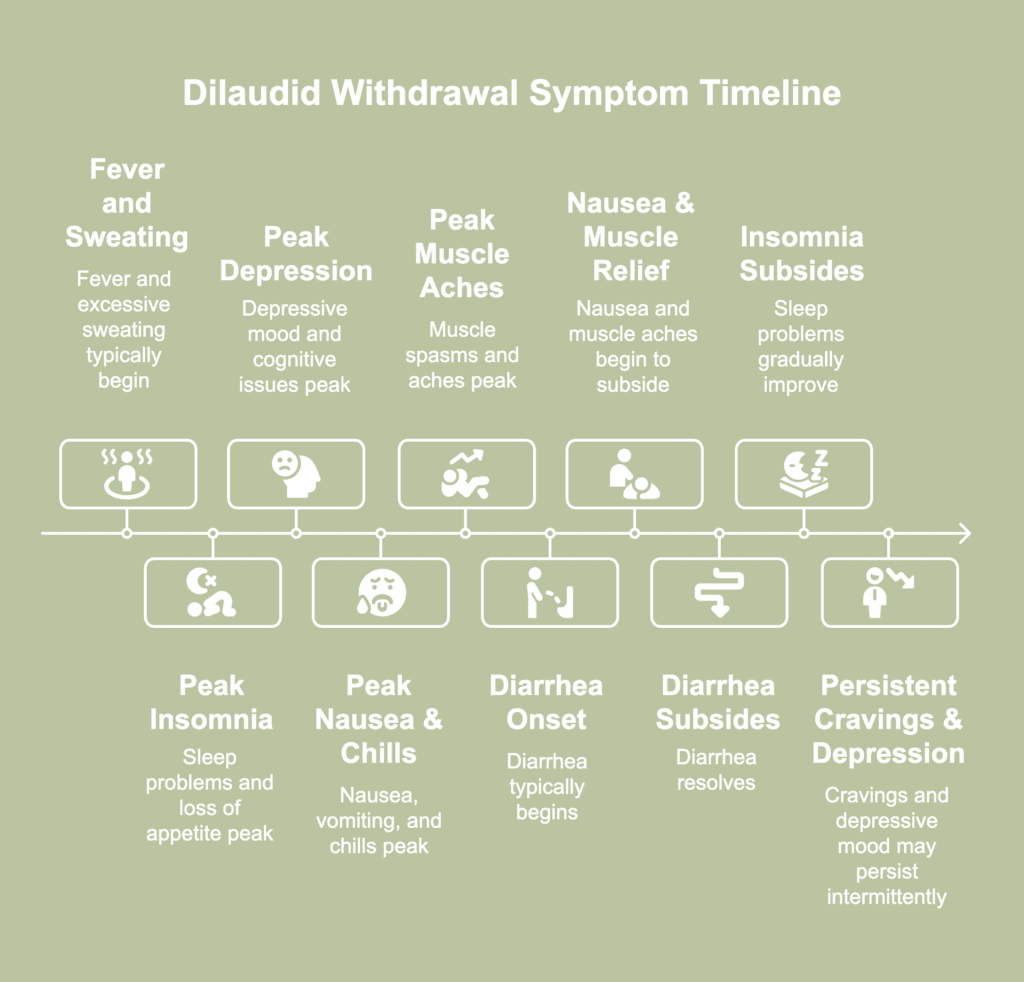
The symptoms of Dilaudid withdrawal are listed below.
- Nausea and vomiting: Symptoms like nausea peak after the first 14 hours of quitting the drug. If intense, these symptoms tend to subside after the third or fourth day of withdrawal.
- Anxiety and restlessness: Symptoms like jitters and anxiety occur during opioid drug withdrawal due to an imbalance of noradrenaline, a chemical linked to increased wakefulness, alertness, blood pressure, and breathing. When the mu-opioid receptors are activated by Dilaudid, they suppress the activity of the neurons that secrete noradrenaline. With increased Dilaudid exposure, the noradrenaline-releasing cells adjust and start producing greater amounts of the chemical. However, during withdrawal, there is no inhibitory effect of Dilaudid to suppress the stimulatory effects of noradrenaline. This results in the manifestation of symptoms like anxiety and restlessness.
- Insomnia: Sleep problems tend to peak within 12-48 hours of stopping drug use. The symptoms persist for 5-14 days, depending on the severity of the addiction problem.
- Fever and sweating: Symptoms like fever and excessive sweating typically manifest within 4-8 hours after stopping Dilaudid.
- Elevated blood pressure and heart rate: These symptoms are caused by an overstimulated nervous system.
- Chills: Shaking and chills tend to peak after the first 14 hours of stopping drug usage.
- Runny nose and/or watery eyes: These symptoms are caused by autonomic hypersensitivity.
- Muscle weakness: The symptoms include muscle spasms, aches, and pains. Muscle aches tend to peak after the first 14 hours of quitting use, and for a section of the population, these symptoms linger faintly till the third or fourth day.
- Loss of appetite: Symptoms like loss of appetite peak within 12-48 hours of stopping Dilaudid. Typically, they begin to lessen in severity after 48-72 hours of drug withdrawal.
- Diarrhea: Diarrhea typically occurs a day after stopping use. It is intense, but resolves within 72 hours.
- Depression: This is a primary symptom of Dilaudid withdrawal that typically peaks within 12-48 hours of quitting the drug. In a section of users, the depressive mood has been observed to persist for weeks and even months, making it challenging for them to sustain recovery.
- Drug cravings: Hydromorphone formulations like Dilaudid possess an increased risk of inducing physical and/or psychological dependence characterized by cravings during withdrawal. A percentage of individuals report experiencing intermittent cravings for weeks and months after they stop using the drug.
- Cognitive issues: These include reduced attention span and impaired memory and problem-solving skills. Individuals experiencing Dilaudid withdrawal have reported mental confusion and a tendency to make poor decisions.
- Suicidal ideation: Scientific literature suggests that the risk of suicidal behavior increases after stopping opioid treatment. The risk is positively correlated with the length of treatment. The triggers include increased pain, sleep issues, the discomfort of the withdrawal process, and exacerbation of co-morbid mental health problems.
