Psychostimulants: uses, side effects, and effectivity


Psychostimulants are psychotropic substances that stimulate the central nervous system and produce effects like enhanced mental and physical functionality, heightened alertness, and prolonged wakefulness. They have significant abuse and addictive potential.
Psychostimulants are used for medicinal and recreational purposes and as physical and cognitive performance enhancers. They are prescribed for conditions like attention-deficit/hyperactivity disorder (ADHD), depression, narcolepsy, and binge-eating disorder.
The side effects of psychostimulants are an elevated heart rate and increased blood pressure, headaches, dizziness and nausea, gastrointestinal issues, reduced appetite, restlessness, anxiety, and insomnia. The severe side effects include psychosis and an increased risk of overdosing on the substance.
Psychostimulants are effective for the majority of ADHD patients and have been shown to reduce core symptoms of the condition in children, adolescents, and adults. These substances are effective in reducing the symptoms of major depressive disorder when used in conjunction with antidepressants and in treating excessive daytime sleepiness associated with narcolepsy.
What are psychostimulants?
Psychostimulants are psychotropic substances that are able to heighten the activity of the central nervous system (CNS). They improve mental and/or physical functionality, and their beneficial effects manifest as increased alertness, wakefulness, enhanced performance, and appetite suppression.
Psychostimulants are prescribed for treating multiple disorders. Specific psychostimulants are used for recreational purposes and have high addiction and abuse potential. Commonly used psychostimulants include legally prescribed medications like methylphenidate and specific amphetamines; illicit drugs like cocaine, methamphetamine, 3-4-methylenedioxymethamphetamine (MDMA or ecstasy), and khat; synthetic stimulants like bath salts; regulated substances like nicotine; and caffeine, which is not controlled.
What are psychostimulants used for?
Psychostimulants are used for medicinal and recreational purposes and to derive performance benefits. They are prescribed for attention-deficit/hyperactivity disorder (ADHD), treatment-resistant depression, narcolepsy, and apathy. They are prescribed as part of a multimodal analgesia regimen to enhance the effects of analgesics. Specific formulations of psychostimulants are used to treat binge-eating disorder. Diet aids like Didrex, Bontril, Fastin, Adipex, Ionamin, Preludin, and Meridia are used to promote weight loss. Common prescription psychostimulants include methylphenidate (Concerta and Ritalin), amphetamines (Adderall and Dexedrine), and armodafinil.
Psychostimulants find off-label use as treatment for stimulant use disorder. Studies of self-report data suggest that controlled prescription psychostimulants like methylphenidate, dextroamphetamine, and modafinil are able to reduce stimulant use and cravings, according to a 2025 article by Suen et al., published in the Journal of Addiction Medicine, titled “Prescribing Psychostimulants for the Treatment of Stimulant Use Disorder: Navigating the Federal Legal Landscape.” However, the prescribing rates of these drugs are low, possibly because of the ambiguities associated with federal laws. The initial promise demonstrated by the efficacy of prescription psychostimulants in treating stimulant use disorder has paved the way for drug trials to assess if these medications have the potential to be used as harm reduction measures in specific populations.
For instance, drug trials are being developed where Adderall will be prescribed to individuals undergoing methadone maintenance treatment and who have co-occurring cocaine dependence, as mentioned by the Drug Policy Alliance in their publication titled “Stimulant Use: Harm Reduction, Treatment, and Future Directions–Conference Report.” The trial will assess the efficacy of Adderall in reducing cocaine use, overdose risk, and HIV risk behaviors.
Prescription stimulants are known to be abused and not used according to a physician’s advice. Other psychostimulants that find use as drugs of abuse include cocaine, methamphetamine, 3-4-methylenedioxymethamphetamine (MDMA or ecstasy), nicotine, and khat. Individuals tend to use these substances to experience euphoric sensations, enhance physical and cognitive performance, increase wakefulness, raise self-esteem, and derive a “high,” as noted by the US Department of Justice and Drug Enforcement Administration in their April 2020 Drug Fact Sheet titled “Stimulants.”
Caffeine, in the form of tea, coffee, chocolate, and energy drinks, has mild stimulant properties and promotes alertness. These caffeine products are often consumed by students and athletes to enhance physical and/or cognitive performance. Athletes are also known to use various formulations of amphetamines to boost physical performance, as stated in a StatPearls [Internet] release by Farzam et al., titled “Stimulants” last updated on 2 July 2023.
How do psychostimulants work?
Psychostimulants work by affecting the central nervous system and influencing the concentration and functionality of critical neurotransmitters like dopamine, norepinephrine, and serotonin. The drug-induced actions of these neurotransmitters trigger multiple excitatory responses across the central nervous system.
The action of psychostimulants on the dopamine transporter significantly contributes to their addiction and abuse potential. Additionally, the neuroadaptations and synaptic plasticity induced by psychostimulant use impair the normal functioning of the dopaminergic reward circuitry, resulting in extended phases of withdrawal marked by negative emotions and cravings. Psychostimulants also act on the neurotransmitters norepinephrine and serotonin to drive drug-seeking behaviors.
As the first-line treatment for ADHD, psychostimulants like methylphenidate and amphetamine treat symptoms like hyperactivity, reduced attention, and impulsivity by restoring the balance between dopamine and norepinephrine, according to a 2010 article by Stephen M. Stahl published in The Journal of Clinical Psychiatry, titled “Mechanism of Action of Stimulants in Attention-Deficit/Hyperactivity Disorder.”
What are the side effects of psychostimulants?

The side effects of psychostimulants are listed below.
- Elevated heart rate and increased blood pressure: CNS stimulants like psychostimulants cause the heart to beat faster and with greater force, thereby potentially increasing blood pressure. Increased sweating is a side effect of psychostimulant use that has been noticed more in male subjects than females, according to a2016 article by Smith et al., published in the journal Substance Use & Misuse, titled “Subjective report of side effects of prescribed and non-prescribed psychostimulant use in young adults.”
- Headaches: Stimulant medications like amphetamines and methylphenidate are associated with headaches, according to a 2021 article by Pan et al., published in the journal Psychological Medicine, titled “Headache in ADHD as comorbidity and a side effect of medications: a systematic review and meta-analysis.”
- Dizziness and nausea: Smith et al. (2016) report that side effects like headaches and nausea are typically reported more by women than men.
- Reduced appetite: Stimulants suppress appetite by increasing dopamine and norepinephrine activity and interacting with the hormonal signals associated with regulating appetite, according to a 2021 article by Antonio Verdejo-Garcia and Rose Crossin published in the journal Neuroscience & Biobehavioral Reviews, titled “Nutritional and metabolic alterations arising from stimulant use: A targeted review of an emerging field.”
- Restlessness, anxiety, and insomnia: These effects are typically associated with an individual emerging from the euphoric “high” of taking stimulants. These effects are generally experienced more by female prescribed and non-prescribed users than males (Smith et al., 2016).
- Stomach aches and diarrhea: Stimulant medications for ADHD are known to cause adverse gastrointestinal symptoms like abdominal pain, bloating, constipation, and increased production of gastric acid that in turn, leads to issues like heartburn and indigestion, according to a 2023 article by Nanda et al., published in the journal Cureus, titled “Adverse Effects of Stimulant Interventions for Attention Deficit Hyperactivity Disorder (ADHD): A Comprehensive Systematic Review.” Adderall is associated with diarrhea.
- Psychosis: Stimulant-induced psychotic disorder (SIPD) is an acute effect of intoxication and manifests as symptoms like delusions and/or hallucinations, according to a 2019 article by Henning et al., published in the journal Cureus, titled “A Case Study of Acute Stimulant-induced Psychosis.” It is associated with the use of methamphetamine and cocaine. Acute psychosis typically occurs within 4-5 days of intoxication and resolves with abstinence. In a percentage of individuals who develop SIPD, symptoms persist for as long as a month. However, individuals are also known to never fully recover from their psychotic symptoms and eventually go on to develop a primary psychotic disorder.
- Aggression: There exists self-report data to suggest that cocaine and methamphetamine use is associated with aggressive and violent behaviors, according to a 2020 article by Kuypers et al., published in the journal European Neuropsychopharmacology, titled “Intoxicated aggression: Do alcohol and stimulants cause dose-related aggression? A review.” Methamphetamine use is linked to increased homicidal behaviors and a tendency to engage in risky, careless, and unsafe driving. These behaviors are likely explained by the increased confidence and lowered inhibition that meth users report. However, a causal link between cocaine and amphetamine use and aggression has not been conclusively proven.
- Overdose: The US Centers for Disease Control and Prevention reports in their web publication titled “Stimulant Overdose” that psychostimulants with abuse potential accounted for 32% of all drug overdose deaths in 2022. Methamphetamine is implicated in the majority of overdose deaths caused by psychostimulants.
What are the long-term effects of psychostimulants?
The long-term effects of psychostimulants are listed below.
- Tooth decay: This is a typical effect of long-term methamphetamine or meth abuse and is colloquially known as “meth mouth.” Chronic methamphetamine use leads to tooth decay and inflammation of oral tissue, which has the possibility of worsening and causing complete tooth loss. The American Dental Association, in its web release titled “Methamphetamine” last updated on 12 July 2023, mentions that methamphetamine abuse causes grinding/clenching of the teeth or bruxism, temporomandibular joint disorders, myofascial pain, and trismus or lockjaw.
- Sores: Chronic methamphetamine users develop sores and abscesses due to their tendency to pick and scratch at their skin. The sores resemble open blisters with a reddish, wet or oozing appearance or scabbed wounds and scars. “Meth mites” is a condition associated with meth sores. Chronic meth users often have tactile hallucinations that cause them to “feel” as if bugs are crawling on or under their skin. They try to scratch at or pick the insects, thereby causing new sores or re-opening and deepening old wounds by repeatedly scratching at the scabs that form over open sores.
- Cognitive deficits: Long-term use of psychostimulants is associated with adverse changes in brain regions implicated in cognitive functions, according to a 2019 article by Manoranjan S. D’Souza published in the journal Frontiers in Psychiatry, titled “Brain and Cognition for Addiction Medicine: From Prevention to Recovery Neural Substrates for Treatment of Psychostimulant-Induced Cognitive Deficits.” Cognitive deficits like impaired memory and learning, poor decision making, and reduced behavioral control have been linked to psychostimulant abuse.
- Increased risk of medical complications: Chronic psychostimulant use is associated with an increased risk of developing severe medical issues like strokes, myocardial infarctions, heart failure, seizures, respiratory problems, and muscular and renal dysfunction.
- Infections: Drug-use habits like injecting stimulants and sharing equipment are associated with an increased risk of developing infectious endocarditis, hepatitis B and C, and AIDS (Acquired immunodeficiency syndrome) caused by HIV (human immunodeficiency virus) infection.
- Onset of a primary psychotic disorder: SIPD is an acute effect of stimulant use. Prolonged and untreated psychosis increases the risk of an individual developing primary psychotic disorder, according to a 2025 article by Lecomte et al., published in the journal Schizophrenia Research: Cognition, titled “SIPD or psychotic disorder with stimulant use.” Primary psychotic disorder is characterized by more severe cognitive deficits than SIPD.
- Loss of libido: According to the findings of a study, male non-prescribed users of psychostimulants tended to report loss of libido more than female participants (Smith et al., 2016).
- Diminished quality of life: Chronic psychostimulant use decreases the quality of life by straining interpersonal relationships, impairing role functioning, increasing employment challenges, reducing motivation, and increasing the risk of homelessness.
- Development of tolerance: It has been observed that tolerance to the effects of stimulants develops within several hours, according to a 2011 article by Jason Yanofski published in the journal Innovations in Clinical Neuroscience, titled “The Dopamine Dilemma—Part II: Could Stimulants Cause Tolerance, Dependence, and Paradoxical Decompensation?” The development of tolerance is caused by neuroadaptive alterations like upregulation of dopamine transporters that decrease drug efficacy, increase of autoreceptor sensitivity, and depletion of neurotransmitters, according to a 2022 article Kenneth Handelman and Fernando Sumiya, published in the journal Brain Sciences, titled “Tolerance to Stimulant Medication for Attention Deficit Hyperactivity Disorder: Literature Review and Case Report.” When tolerance develops, individuals take increased amounts of the stimulant to feel the earlier magnitude of effects.
- Withdrawal syndrome: The majority of cocaine and meth users experience withdrawal symptoms when they stop using the substance or reduce dosage, according to a 2022 article by Michael J. Li and Steven J. Shoptaw published in the journal Addiction, titled “Clinical Management of Psychostimulant Withdrawal: Review of the Evidence.” The typical psychostimulant withdrawal symptoms are cravings, depression, anhedonia, anxiety, irritability, headaches, pain, fatigue, prolonged sleep, and reduced focus. The manifestation of withdrawal symptoms upon abstinence indicates physical dependence.
- Development of addiction: Withdrawal symptoms are uncomfortable and stressful, compelling individuals to restart using the drug to escape the discomfort. This marks the beginning of compulsive and uncontrollable drug use that is a hallmark of addiction.
What are the effects of psychostimulants in the brain?
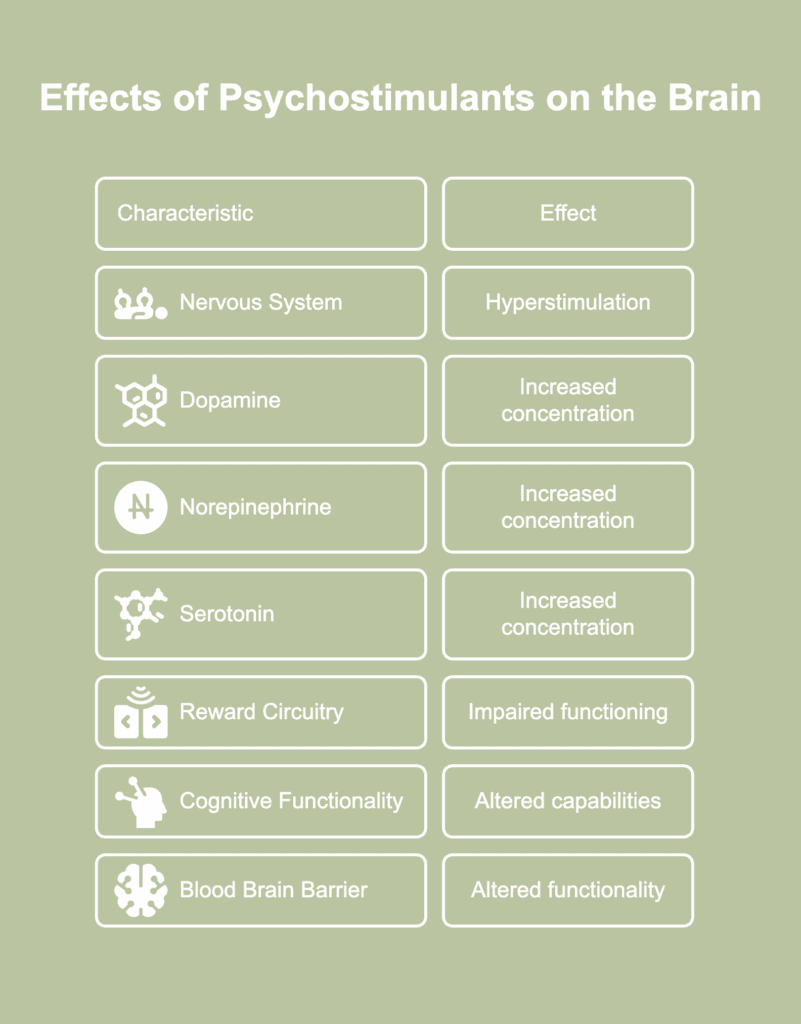
The effects of psychostimulants in the brain are listed below.
- Hyperstimulation of the nervous system: Psychostimulants hyperstimulate the CNS by increasing sympathetic nervous system activity. Hyperstimulation of the CNS manifests as characteristic stimulant effects like increased energy, focus, and alertness.
- Increased concentration of dopamine: Psychostimulants increase the level of dopamine in the brain, especially in limbic regions such as the nucleus accumbens, according to a 2015 article by Peña et al., published in the European Journal of Pharmacology, titled “Psychostimulants affect dopamine transmission through both dopamine transporter-dependent and independent mechanisms.” Cocaine and methylphenidate produce this effect by binding to the dopamine transporter and preventing the reuptake of the neurotransmitter. Amphetamine increases dopamine concentration by triggering the release of dopamine as well as by disrupting its reuptake. This increase in dopamine contributes to the reinforcing effects of psychostimulants.
- Increased concentration of norepinephrine: Psychostimulants increase the levels of norepinephrine in the prefrontal cortex (Peña et al., 2015). The perception of the rewarding effects of psychostimulants is mediated by the synaptic concentration of both dopamine and norepinephrine. The noradrenergic system, mediated by norepinephrine, is implicated in arousal, attention, memory, learning, mood, and stress response. Besides mediating reward saliency, norepinephrine is also critically involved in triggering stimulant effects like drug desensitization and reinstatement of drug-seeking behaviors.
- Increased concentration of serotonin: The majority of psychostimulants with addictive potential increase the concentration of serotonin in large areas of the brain by binding to the serotonin transporter, thereby inhibiting neurotransmitter reuptake and increasing extracellular serotonin outflow, according to a 2021 article by Ewa Taracha published in the journal Postepy Psychiatrii i Neurologii, titled “The role of serotoninergic system in psychostimulant effects.”Serotonin is linked to associative learning, which in the context of addiction, is a mechanism that influences the transition from intermittent and controlled drug use, via abuse, to uncontrolled and compulsive substance-taking behaviors.
- Impaired functioning of the reward circuitry: The dopamine-mediated reward system of the brain extends across the ventral tegmental area (VTA), the nucleus accumbens (NAc), and the prefrontal cortex. Psychostimulants stimulate dopaminergic activity in the VTA and NAc to mediate initial drug-seeking tendencies. Additionally, these substances dysregulate prefrontal control of the NAc, thereby impairing the normal functionality of the reward circuitry. Psychostimulants alter gene expression and influence processes in the reward system associated with mitochondrial function and synaptic plasticity that are known to contribute to drug-seeking behaviors, according to a 2023 article by Rianne R. Campbell and Mary Kay Lobo published in the journal Current Opinion in Neurobiology, titled “Neurobiological mechanisms underlying psychostimulant use.”
- Alteration of cognitive functionality: Psychostimulants have been observed to improve cognitive capabilities, such as memory, divided attention, and focused attention, in ADHD patients, according to a 2022 article by McKenzie et al., published in the Journal of Psychiatric Research, titled “The effects of psychostimulants on cognitive functions in individuals with attention-deficit hyperactivity disorder: A systematic review.” However, these procognitive effects are only associated with low doses of psychostimulants. Imaging studies of chronic meth users show gray matter volume loss in cortical areas, such as the frontal, insular, cingulate, temporal, and occipital cortices. Chronic cocaine and amphetamine users show decreased gray matter in the ventromedial prefrontal cortex, inferior frontal gyrus, pregenual anterior cingulate gyrus, insula, and anterior thalamus, as noted in the chapter “How Stimulants Affect the Brain and Behavior” from the SAMHSA (Substance Abuse and Mental Health Services Administration) publication titled “Treatment for Stimulant Use Disorders: Updated 2021 [Internet].” It is believed that psychostimulant abuse causes loss of neurons in the hippocampus, a critical area associated with learning.
- Altered functionality of the blood brain barrier: Studies show that psychostimulants like methamphetamine, MDMA, and cocaine compromise the integrity of the blood brain barrier (BBB) by a cascade of mechanisms like altering protein expression, stimulating neuroinflammatory pathways, activating specific enzymes, according to a 2012 article by Kousik et al., published in the journal Frontiers in Pharmacology, titled “The effects of psychostimulant drugs on blood brain barrier function and neuroinflammation.” Damage to the BBB increases the permeability of the membrane. The brain thus becomes vulnerable to the invasion of peripheral toxins, a development that is associated with cocaine and meth abuse.
How effective are psychostimulants?
Psychostimulants are effective for the majority of patients–children, adolescents, and adults– who take it for treating ADHD, according to a 2022 article Kenneth Handelman and Fernando Sumiya, published in the journal Brain Sciences, titled “Tolerance to Stimulant Medication for Attention Deficit Hyperactivity Disorder: Literature Review and Case Report.” A psychostimulant treatment regimen comprising methylphenidate followed by dexamphetamines reduces ADHD symptoms in 70% of patients, according to a 2014 article by Rubia et al., published in the journal Biological Psychiatry, titled “Effects of Stimulants on Brain Function in Attention-Deficit/Hyperactivity Disorder: A Systematic Review and Meta-Analysis.” There is robust scientific evidence to suggest that psychostimulants are able to reduce core symptoms of ADHD, such as inattention, impulsivity, and hyperactivity, in children and adolescents, according to a 2022 article by Mechler et al., published in the journal Pharmacology & Therapeutics, titled “Evidence-based pharmacological treatment options for ADHD in children and adolescents.”
It has been observed that individuals with depression exhibited a statistically significant improvement in symptoms after being administered psychostimulants alongside antidepressants, according to a 2023 article by Janela et al., published in the journal Current Treatment Options in Psychiatry, titled “Psychostimulant Augmentation of Antidepressant Therapy in Depression: a Systematic Review and Meta-Analysis.” Methylphenidate, amphetamine, methamphetamine, and dextroamphetamine are effective in treating narcolepsy symptoms like excessive daytime sleepiness, according to a 2019 publication by Moshe Turner featured in the Journal of Clinical Sleep Medicine, titled “The Treatment of Narcolepsy With Amphetamine-Based Stimulant Medications: A Call for Better Understanding.”
Authors Tardelli et al., in a 2020 article titled “Prescription psychostimulants for the treatment of stimulant use disorder: a systematic review and meta-analysis” and published in the journal Psychopharmacology, mention that prescription amphetamines in large doses produce clinically significant abstinence benefits in individuals with stimulant use disorder, especially cocaine dependence.
Who can prescribe psychostimulants?
Psychostimulants can be prescribed by specialist prescribers like psychiatrists, neurologists, and pediatricians. In countries like Australia, these professionals are authorized under a class authority to prescribe these drugs for treating ADHD in individuals who are not drug-dependent. This means that they are not required to seek approval to prescribe the drugs for individual patients.
However, it is likely that they have to apply for individual patient approval to prescribe psychostimulants to drug-dependent individuals, treat conditions other than ADHD, and in doses that exceed a specified amount for specific ADHD medications. In countries like the US, psychostimulants are prescribed by psychiatrists, neurologists, pediatricians, primary care physicians, nurse practitioners, and physician assistants who are supervised by a physician.
In Canada, psychostimulants are prescribed to individuals with stimulant use disorder by general physicians, addiction medicine specialists, and nurse practitioners, according to a 2023 article by Heather Palis and Scott MacDonald published in the Canadian Medical Association Journal, titled “Incorporating prescription psychostimulants into the continuum of care for people with stimulant use disorder in Canada.” It has been observed that psychostimulants are mostly prescribed by physicians who are already working with patients with substance use disorders.
What are alternatives for psychostimulants?
The alternatives for psychostimulants are listed below.
- Non-stimulant medications: Non-stimulant medications do not contain methylphenidate or amphetamine and hence, are unable to cause the adverse effects associated with stimulant use. They work on different neurotransmitter pathways in the brain (such as norepinephrine), unlike stimulant medications that target the dopamine system. However, they produce therapeutic benefits comparable to those associated with stimulant medications. Examples of non-stimulant medications include atomoxetine (Strattera), viloxazine (Qelbree), and alpha-2 adrenergic agonists (clonidine and guanfacine). Non-stimulant medications are used when stimulant drugs are not tolerated, fail to produce desired therapeutic benefits, or the patient is drug-dependent or has a history of substance abuse. These medications are appropriate for patients who have a co-occurring condition that is likely to be worsened by a stimulant medicine.
- Bupropion: Bupropion (Wellbutrin and Zyban) is an antidepressant and a weak and indirect dopamine agonist. It works by blocking dopamine transporters, thereby increasing the extracellular concentration of dopamine. It produces mild amphetamine-like effects, especially when it is injected or breathed in.
- Tricyclic antidepressants: Tricyclic antidepressants (TCAs) are used to treat major depressive disorder. Although not classified as stimulants, they produce stimulant-like effects by their action on the norepinephrine system. TCAs prevent the reuptake of norepinephrine, thereby prolonging the presence of this neurotransmitter in the synapse. An increased activity of norepinephrine is associated with CNS stimulation that manifests as increased energy, attention, and wakefulness.
- Serotonin norepinephrine reuptake inhibitors (SNRIs): SNRIs like desvenlafaxine (Khedezla and Pristiq), duloxetine (Drizalma, Irenka, and Cymbalta), levomilnacipran (Fetzima), milnacipran (Savella), and venlafaxine (Effexor) are antidepressants that work by blocking the reuptake of serotonin and norepinephrine. Serotonin is associated with appetite, social interactions, and libido. Norepinephrine regulates alertness and attention levels. By keeping these neurotransmitters active in the brain, SNRIs produce stimulant-like effects, such as increased nervous system arousal.
- Central anticholinesterases: These drugs prolong the presence of acetylcholine in the nervous system. Acetylcholine is an excitatory neurotransmitter. It is implicated in attention and arousal. The increased availability and activity of acetylcholine over stimulates the parasympathetic nervous system and triggers adverse effects like headaches, abdominal cramps, and increased blood pressure that resemble the side effects caused by stimulants.
Are psychostimulants addictive?
Yes, psychostimulants are addictive because they have the ability to influence the brain’s reward system and induce neural and functional changes. These changes in the brain drive compulsive drug-seeking behaviors and trigger the development of tolerance, dependence, and withdrawal, resulting in the maintenance and relapse of addiction. The abuse and addiction potential of psychostimulants varies. Cocaine is believed to be the most addictive stimulant in the world, followed by methamphetamine. Even prescription stimulants possess the risk of misuse, addiction, overdose, and diversion. For instance, intravenous administration of methylphenidate is known to induce euphoric feelings that mimic those produced by cocaine. They are classified as Schedule II drugs per the Controlled Substances Act, as stated by the Food and Drug Administration (FDA) in its publication titled “Prescription Stimulant Medications” last updated on 29 July 2024.
The data collected from the 2015 and 2016 National Surveys on Drug Use and Health and presented in the 2018 article by Compton et al., published in the American Journal of Psychiatry, titled “Prevalence and Correlates of Prescription Stimulant Use, Misuse, Use Disorders, and Motivations for Misuse Among Adults in the United States” reveals the prevalence of stimulant addiction. An estimated 0.2% of American adults, or 0.4 million individuals, were found to be addicted to prescription stimulants. In 2022, 35 million individuals worldwide were found to meet the criteria for stimulant addiction associated with amphetamines, cocaine, and MDMA.
