Antiepileptic agents: definition, use, and side effects


Table of content
- What are antiepileptic agents?
- What are antiepileptic agents used for?
- How do antiepileptic agents work?
- What are examples of antiepileptic agents?
- What are the side effects of antiepileptic agents?
- How effective are antiepileptic agents?
- How fast do antiepileptic agents work?
- How are antiepileptic agents administered?
- Do you need a prescription for antiepileptic agents?
- Are antiepileptic agents addictive?
Antiepileptic agents are medications that help treat epilepsy and seizures induced by other conditions.
Antiepileptic agents are used primarily to prevent and manage seizures associated with epilepsy and other causes. They are used to manage systems of anxiety, bipolar disorder, neuropathic pain, and Parkinson’s disease.
The side effects of antiepileptic drugs are headaches, fatigue, dizziness, blurred vision, sleepiness, nausea and vomiting, and cutaneous reactions like rashes. These drugs are known to cause adverse effects like cognitive impairment, psychiatric and behavioral problems, bone disorders, and hematological complications.
What are antiepileptic agents?
Antiepileptic agents are a class of drugs used to prevent or treat seizures or convulsions associated with epilepsy or other conditions. These medications are used to prevent the onset and decrease the frequency and severity of seizures. They do not cure epilepsy.
What are the other names for antiepileptic agents?
The other names for antiepileptic agents are anticonvulsant drugs and antiseizure medications. The use of the term “antiseizure”is recommended by the International League Against Epilepsy as it is the most accurate representation of the primary action of the antiepileptic drugs currently in use, which is to produce a symptomatic effect against seizures. The term “antiepileptic” is misleading because these drugs do not directly address the underlying cause of the seizures.
What are antiepileptic agents used for?
Antiepileptic agents are primarily used for managing epilepsy and treating other causes of seizures. These drugs are used to prevent the onset of and/or treat seizures during or after brain surgery. They are also prescribed for neurological and psychiatric conditions not related to epilepsy. The US Food and Drug Administration (FDA) approves the use of specific formulations of antiepileptic drugs to treat migraine, neuropathic pain, and mania in adults. Antiepileptic drugs are believed to treat anxiety, bipolar disorder, fibromyalgia, Parkinson’s disease, and restless leg syndrome. Topiramate and zonisamide are prescribed to promote weight loss.
How do antiepileptic agents work?
Antiepileptic agents work to prevent seizures by regulating abnormal electrical activity in the brain caused by an imbalance between excitatory and inhibitory circuits. Epileptic seizures are generated when this imbalance favors neuronal excitation over inhibition. Antiepileptic drugs aim to produce inhibition of the excitatory action or strengthening of the inhibitory action, or both, according to a 2021 article by Tahir Hakami published in the journal Neuropsychopharmacology Report, titled “Neuropharmacology of Antiseizure Drugs.”
The opening and closing of ion channels causes a cell to fire. Antiepileptic medications directly affect the opening and closing of specific ion channels by acting on sodium and calcium ion channel blockers and potassium channel openers. Alternatively, these drugs indirectly influence the workings of specific ion channels by modulating the synthesis, metabolism, and actions of neurotransmitters and receptors that in turn, regulate channel opening and closing, as explained in the chapter “Neuropharmacology of Antiepileptic Drugs” in the 2006 publication by the American Epilepsy Society titled “An Introduction to Epilepsy [Internet]” The indirect actions are enhancing the power of the inhibitory GABA (gamma-aminobutyric acid) neurotransmission system; reducing the excitatory activity of glutamate; and regulating presynaptic neurotransmitter release.
Drugs like topiramate and felbamate have multiple modes of action. For instance, topiramate acts on the sodium channel and the GABA receptor. Felbamate works on the GABA and glutamate receptors. The exact mechanism of action of rufinamide, zonisamide, and valproate is not yet known (Hakami, 2021).
What are examples of antiepileptic agents?
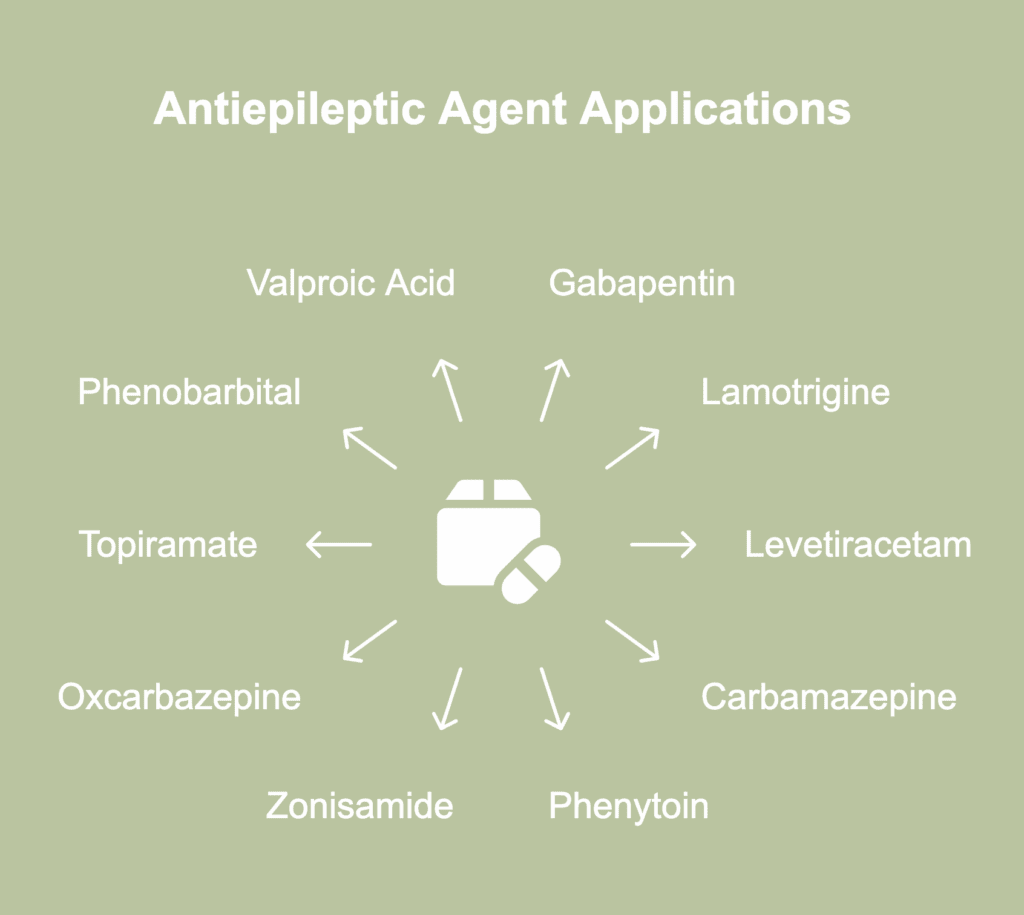
The examples of antiepileptic agents are listed below.
- Gabapentin (Neurontin): Gabapentin is effective as an adjunct treatment for partial seizures in adults and children aged 3 years and older. It is also used to manage restless leg syndrome; specific types of neural pain, such as that caused by shingles; and psychiatric illnesses.
- Lamotrigine (Lamictal): Lamotrigine calms brain activity and helps manage partial seizures, primary generalized tonic-clonic seizures, and Lennox-Gastaut syndrome. It is effective in managing mood changes associated with bipolar disorder. It has off-label use as a treatment for acute bipolar depression, unipolar depression, fibromyalgia, and schizophrenia.
- Levetiracetam (Keppra, Spritam, Elepsia, Roweepra): Levetiracetam is used to treat focal-onset seizures in patients 1 month and older; primary generalized tonic-clonic seizures in patients 6 years and older with idiopathic generalized epilepsy; and myoclonic seizures in patients aged 12 years or more who have been diagnosed with juvenile myoclonic epilepsy.
- Carbamazepine (Tegretol): Carbamazepine decreases nerve impulses that trigger seizures and pain. It is used to treat partial seizures with complex symptoms; generalized tonic-clonic seizures; mixed seizures; nerve pain caused by trigeminal neuralgia and glossopharyngeal neuralgia; and manic episodes and mixed manic-depressive episodes associated with bipolar I disorder.
- Phenytoin (Dilantin): Phenytoin is used to manage and treat epilepsy, complex partial seizures, generalized tonic-clonic seizures, and status epilepticus. It is used to treat or prevent the onset of seizures that begin during or after a surgery of the brain or nervous system.
- Zonisamide (Zonegran, Zonisade): Zonisamide is used as an adjunct therapy for the treatment of partial or focal seizures in patients older than 16 years. It has off-label use as a treatment for neuropathic pain.
- Oxcarbazepine (Trileptal, Oxtellar XR): Oxcarbazepine is used to treat partial seizures associated with epilepsy in adults and children aged between 4 and 16 years. It is listed as a first-line or second-line treatment for primary generalized tonic-clonic seizures and focal-onset epilepsy in multiple countries around the world. It has off-label use as a treatment for bipolar disorder and trigeminal neuralgia in individuals with multiple sclerosis.
- Topiramate (Topamax): Topiramate is used to treat partial seizures, primary generalized tonic-clonic seizures, and seizures associated with Lennox-Gastaut syndrome in adults and children aged 2 years or more. It is prescribed as monotherapy or alongside other antiepileptic medications. It is used to prevent the onset of migraine headaches.
- Phenobarbital ( Solfoton, Luminal, Sezaby ): Phenobarbital is a sedative-hypnotic substance that belongs to the barbiturate group of drugs. It is used as an anti-seizure medication to treat and/or prevent seizures in patients with epilepsy and as treatment for status epilepticus. However, it has not been approved by the FDA as an anticonvulsant medication.
- Valproic acid: The FDA has approved the use of valproic acid to treat absence seizures or petit mal seizures and complex partial seizures, alternatively known as psychomotor seizures. It is one of the most commonly prescribed antiepileptic drugs. It is also effective at managing migraine and bipolar disorder.
What are the side effects of antiepileptic agents?
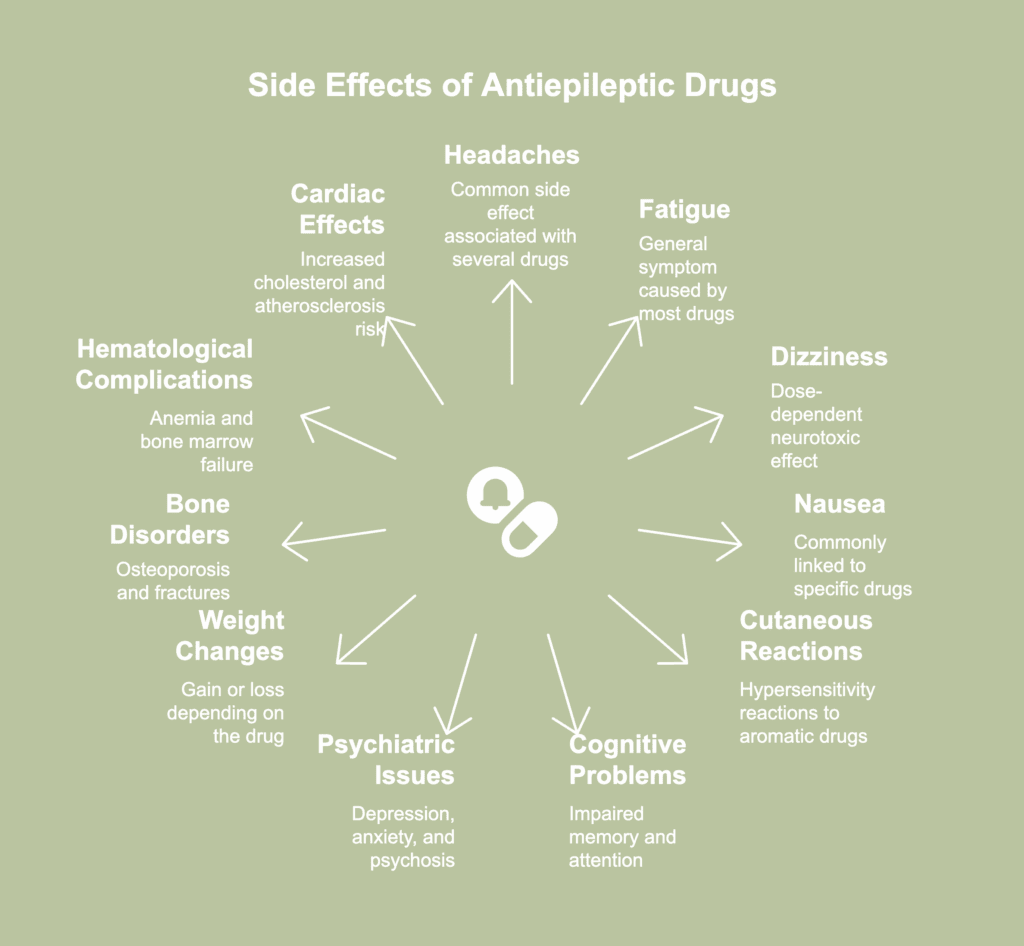
The side effects of antiepileptic agents are listed below.
- Headaches: Rufinamide, lacosamide, oxcarbazepine, levetiracetam, and lamotrigine are associated with headaches.
- Fatigue and sleepiness: The majority of antiepileptic drugs are known to cause these general symptoms.
- Dizziness and blurred vision: All antiepileptic agents have the potential to cause dose-dependent neurotoxic effects like dizziness, blurred vision, and uncoordinated movements, especially at the start of therapy and with polytherapy, according to a 2009 article by E. K. St. Louis published in the journal Current Neuropharmacology, titled “Minimizing AED Adverse Effects: Improving Quality of Life in the Interictal State in Epilepsy Care.”
- Nausea and vomiting: Felbamate, valproic acid, lamotrigine, topiramate, ethosuximide, carbamazepine, oxcarbazepine, and rufinamide are commonly associated with nausea and vomiting. Antiepileptic drugs are known to cause other gastrointestinal side effects, like anorexia or increased appetite.
- Cutaneous reactions: Aromatic antiepileptic drugs like phenytoin, carbamazepine, phenobarbital, and lamotrigine have been observed to trigger cutaneous hypersensitivity reactions, according to a 2019 article by Park et al., published in the journal Allergy, Asthma & Immunology Research, titled “Severe Cutaneous Adverse Reactions to Antiepileptic Drugs: A Nationwide Registry-Based Study in Korea.” The symptoms range from minor skin rashes to rare but severe manifestations like Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) that cause significant morbidity and mortality.
- Cognitive problems: The effects include impaired memory, reduced attention, problems with language like struggling to find the right words to communicate, difficulty with planning and reasoning, and abnormal delays in task performance, according to a 2020 article by Mutanana et al., published in the African Journal of Primary Health Care & Family Medicine, titled “General side effects and challenges associated with anti-epilepsy medication: A review of related literature.” Antiepileptic drugs reduce the excitability of neurons or enhance inhibitory neurotransmission, thereby causing these cognitive problems. Typically, older medications like phenobarbital are associated with cognitive problems. However, the newer drug topiramate has been found to carry the greatest risk of cognitive impairment among all similar agents, according to a 2008 article by Sung-Pa Park and Soon-Hak Kwon published in the Journal of Clinical Neurology, titled “Cognitive Effects of Antiepileptic Drugs.”
- Psychiatric and behavioral problems: Levetiracetam and zonisamide have been implicated in adverse psychotropic effects like depression, anxiety, and psychosis, according to a 2025 article by Gandy et al., published in the journal Epilepsy & Behavior, titled “Providing integrated mental health care as a neurologist.” Aggression and homicidal tendencies have been reported with perampanel. It has been observed that a history of mental health disorders and having absence seizures, secondary generalized seizures, and intractable epilepsy increase the risk of developing psychiatric problems in patients who take antiepileptic drugs, according to a 2017 article by Chen et al., published in the journal Epilepsy & Behavior, titled “Psychiatric and behavioral side effects of antiepileptic drugs in adults with epilepsy.” Gandy et al., suggest that antiepileptic drugs have the potential to interact with psychotropic medicines and influence their metabolism, thereby resulting in a recurrence of symptoms.
- Weight gain or loss: Valproate has been associated with weight gain in teenagers and adults. However, very young children being treated with valproate tend to exhibit weight loss. Other antiepileptic agents linked to weight gain are carbamazepine, gabapentin, and pregabalin. On the other hand, felbamate, topiramate, and zonisamide are associated with weight loss.
- Bone disorders: Phenytoin, primidone, and phenobarbital are associated with bone disorders like osteopenia/osteoporosis, osteomalacia, and fractures, according to a 2001 article by Pack et al., published in the journal CNS Drugs, titled “Adverse effects of antiepileptic drugs on bone structure: epidemiology, mechanisms and therapeutic implications.” Specific populations like children, postmenopausal women, elderly men, and hospitalized patients are at an increased risk of developing bone disorders associated with antiepileptic drugs.
- Hematological complications: Older antiepileptic drugs like carbamazepine, phenytoin, and valproic acid have been linked to the development of hematological disorders like mild thrombocytopenia or neutropenia, anemia, red cell aplasia, and bone marrow failure in severe cases, according to a 2014 article by Verrotti et al., published in the journal Neurological Sciences, titled “Anticonvulsant drugs and hematological disease.”
- Cardiac effects: Enzyme-inducing antiepileptic drugs like phenytoin, carbamazepine, and phenobarbital have been observed to produce adverse cardiac effects like increasing total cholesterol and low-density lipoprotein (LDL) levels and elevating the risk of developing atherosclerosis, according to a 2025 article by Abbasi et al., published in the journal Epilepsy & Behavior Reports, titled “Antiseizure medications and their differing effects on cardiovascular risk.”
How effective are antiepileptic agents?

Antiepileptic agents are highly effective because it has been observed that up to 70% of patients with epilepsy tend to become seizure-free with the administration of the optimum antiepileptic medication, according to a 2004 article by Josemir W. Sander published in the journal Epilepsia, titled “The use of antiepileptic drugs–principles and practice.” The remaining 30% of epilepsy patients are extremely challenging to treat.
The majority of the patients who achieve seizure control do so with the first or second drug regimen, as noted by Chen et al., in a 2018 article titled “Treatment Outcomes in Patients With Newly Diagnosed Epilepsy Treated With Established and New Antiepileptic Drugs–A 30-Year Longitudinal Cohort Study” published in the journal JAMA Neurology. The probability of gaining seizure freedom decreases significantly with every subsequent drug regimen implemented. The efficacy of antiepileptic agents depends on choosing a formulation that is effective against the specific type of seizure the patient experiences and their epilepsy syndrome, and strikes a balance between providing optimal seizure control while triggering minimal adverse effects. It must also be noted that 25-30% of patients have drug-resistant epilepsy that does not respond to antiepileptic medications administered alone or in combination with other formulations.
It must be noted that antiepileptic medications are able to reduce the frequency of onset, severity, and duration of seizures. They cannot cure epilepsy. It has also been found that treatment with first-generation drugs tends to fail in 30-40% of patients with new-onset epilepsy due to severe adverse effects, according to a 2021 article by Tahir Hakami published in the journal Therapeutic Advances in Neurological Disorders, titled “Efficacy and tolerability of antiseizure drugs.”
On average, about two-thirds of the patients with new-onset epilepsy who were treated with new antiepileptic drugs showed greater remission rates compared to the results achieved with older drugs, according to a 2011 article by Dieter Schmidt published in the journal Epilepsy Current, titled “Efficacy of New Antiepileptic Drugs.” A number of second-generation antiepileptic drugs have greater tolerability and improved safety profiles compared to older medications, especially for treating women of childbearing potential and elderly patients. However, they are not more effective than their predecessors.
Can antiepileptic agents treat mental illnesses?
Yes, antiepileptic agents can treat specific mental illnesses like bipolar disorder by managing their symptoms. Carbamazepine extended-release has been approved by the FDA as a therapy for acute manic and mixed episodes associated with bipolar I disorder, according to a StatPearls [Internet] release by Maan et al., titled “Carbamazepine” last updated on 10 July 2023. Valproic acid has off-label use for treating mania associated with bipolar disorder, according to a StatPearls [Internet] release titled “Valproic Acid” by Rahman et al., last updated on 19 March 2024.
Antiepileptic drugs suppress seizures or dampen the brain’s heightened electrical activity during the period between seizures. These effects have the ability to confer both positive and negative psychiatric benefits, according to a 2005 article by Siddhartha Nadkarni and Orrin Devinsky published in the journal Epileptic Currents, titled “Psychotropic Effects of Antiepileptic Drugs.” For instance, valproic acid and carbamazepine have the potential to trigger depression and reduce attention. Although felbamate and lamotrigine possess antidepressant and attention-enhancing properties, they are associated with anxiety, agitation, and insomnia. It must be noted that the majority of antiepileptic drugs are prescribed off-label for childhood mental illness.
How fast do antiepileptic agents work?
Antiepileptic agents work extremely fast–within a few seconds–or comparatively slowly, with an onset of action ranging from a few hours to several months, depending on the form of medication, its half-life, and route of administration. For instance, medications that come as immediate-release capsules or tablets start to work within hours of administration. Drugs with longer half-lives, when taken regularly, start to show therapeutic effects after several months.
Situations when a seizure continues for 5 minutes or more (a condition known as status epilepticus or SE) or when SE occurs during a convulsive or tonic-clonic seizure are considered emergencies. The first-line treatment for early SE is benzodiazepine anticonvulsants, such as lorazepam, diazepam, and midazolam, according to a 2020 article by Kim et al., published in the Journal of Clinical Neurology, titled “Antiepileptic Drug Therapy for Status Epilepticus.” Both lorazepam and diazepam typically have an onset of action within 1-3 minutes when administered intravenously. Repeat doses are administered after 3-5 minutes if seizures fail to stop after the first dose.Frequently used antiepileptic drugs like levetiracetam, fosphenytoin, and valproate have been observed to halt status epilepticus and improve consciousness within 60 minutes of administration in 47%, 45%, and 46% of patients, respectively (Kim et al., 2020).
How are antiepileptic agents administered?
Antiepileptic agents are typically administered through the oral route. These drugs are also administered intravenously, intramuscularly, or rectally. Intravenous push administration of antiepileptic drugs is a frequently used procedure in emergency situations. If the oral route is unavailable, medications are administered via the intranasal, buccal, or sublingual routes.
Do you need a prescription for antiepileptic agents?
Yes, you need a prescription for antiepileptic agents from a licensed healthcare practitioner. Physicians prescribe these medications after considering factors like the type of seizure, the patient’s age, side effects of the agent, and other medications that the patient is taking.
Can antiepileptic agents be prescribed alongside other medications?
Yes, antiepileptic agents can be prescribed alongside other medications. Clinically significant drug interactions are possible when antiepileptic agents are used alongside other medications, including different formulations of antiepileptic drugs. So, it is imperative that patients seeking epilepsy treatment inform their physicians about the medications they are currently taking. Patients taking antiepileptic agents should inform their physicians before starting any new medication.
What drugs interact with antiepileptic agents?
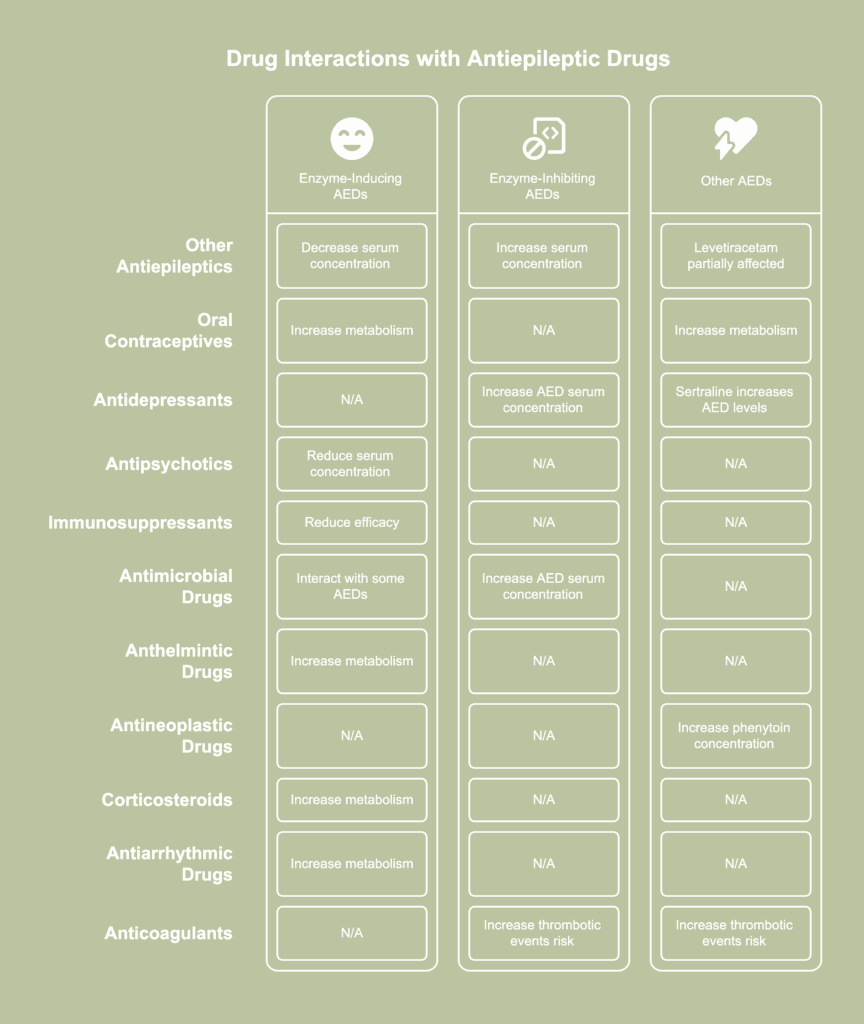
The drugs that interact with antiepileptic agents are listed below.
- Other antiepileptic drugs: Enzyme-inducing antiepileptic drugs are known to increase the metabolism rate, thereby decreasing the half-life, of the majority of co-administered antiepileptic drugs like valproic acid, ethosuximide, felbamate, lamotrigine, tiagabine, topiramate, oxcarbazepine and its monohydroxy-derivative, zonisamide, several benzodiazepines and, to a partial degree, levetiracetam, according to a 2010 article by Svein I. Johannessen and Cecilie Johannessen Landmark published in the journal Current Neuropharmacology, titled “Antiepileptic Drug Interactions – Principles and Clinical Implications.” The principal enzyme-inducing antiepileptic drugs are carbamazepine, phenobarbital, phenytoin, and primidone.However, the reduction in the serum concentration of the affected drug, and thus a decrease in its efficacy, is compensated for by the effect of the inducing drug. On the other hand, enzyme-inhibiting antiepileptic drugs like valproic acid, felbamate, oxcarbazepine, and stiripentol increase the serum concentration of several co-administered antiepileptic agents. The affected drugs include lamotrigine, phenobarbital, carbamazepine, phenytoin, clobazam, and rufinamide. An increase in serum concentration increases the risk of drug-induced toxicity.
- Oral contraceptives: First-generation antiepileptic drugs and newer agents like oxcarbazepine, lamotrigine, felbamate, topiramate in doses greater than 200 mg, rufinamide, and eslicarbazepine acetate increase the metabolism of oral hormonal contraceptives (Johannessen and Johannessen, 2010).
- Antidepressants: Antidepressants like fluoxetine, fluvoxamine, nefazodone, trazodone, and viloxazine are known to increase the serum concentration of antiepileptic agents like carbamazepine by reducing the latter’s rate of metabolism, according to a 2005 article by Emilio Perucca published in the British Journal of Clinical Pharmacology, titled “Clinically relevant drug interactions with antiepileptic drugs.” The antidepressant sertraline increases the serum concentration of lamotrigine, phenytoin, and valproic acid. The metabolism of phenytoin is inhibited by antidepressants like fluoxetine, fluvoxamine, imipramine, trazodone, and viloxazine.
- Antipsychotics : Enzyme-inducing antiepileptic drugs reduce the serum concentration of antipsychotics, thereby decreasing their therapeutic efficacy. For instance, phenobarbital affects clozapine, haloperidol, and chlorpromazine. Phenytoin affects quetiapine, clozapine, haloperidol, and chlorpromazine. Carbamazepine affects older typical and newer atypical antipsychotics like risperidone, clozapine, olanzapine, quetiapine, ziprasidone, aripiprazole, haloperidol, and chlorpromazine (Johannessen and Johannessen, 2010).
- Immunosuppressants: Phenytoin, carbamazepine, and phenobarbital are likely to reduce the efficacy of immunosuppressants like calcineurin inhibitors, according to a 2006 article by Rosemary Cross published in the journal Pharmacy Times, titled “Transplant Immunosuppressants: Common Drug Interactions.”
- Antimicrobial drugs: The antimicrobial drug isoniazid increases the serum concentration of antiepileptic drugs like valproic acid, phenytoin, ethosuximide, and carbamazepine (Perucca, 2005). Chloramphenicol increases the serum concentration of phenobarbital and phenytoin. Additionally, antimicrobials like clarithromycin, erythromycin, fluconazole, ketoconazole, metronidazole, miconazole, sulfaphenazole, ritonavir, and troleandomycin are known to interact with antiepileptic agents like carbamazepine and phenytoin.
- Anthelmintic drugs: Phenytoin, phenobarbital, and carbamazepine are known to increase the rate of metabolism of the anthelmintic drugs praziquantel and albendazole, which are used to treat parasitic infections, according to a 2008 article by Joy Desai published in the journal Epilepsia, titled “Perspectives on interactions between antiepileptic drugs (AEDs) and antimicrobial agents.” This interaction is likely to trigger therapeutic failure of the affected drugs.
- Antineoplastic drugs: Antineoplastic or chemotherapy drugs like doxifluridine, fluorouracil, tamoxifen, tegafur, and UFT (combination of tegafur and uracil)are known to increase the serum concentration of phenytoin (Perucca, 2005).
- Corticosteroids: Carbamazepine, barbiturates, and phenytoin are known to increase the rate of metabolism of corticosteroids like cortisol, hydrocortisone, dexamethasone, methylprednisolone, prednisone, and prednisolone, according to a 2003 article by Philip N. Patsalos and Emilio Perucca published in the journal The Lancet Neurology, titled “Clinically important drug interactions in epilepsy: interactions between antiepileptic drugs and other drugs.” This reduces the therapeutic efficacy of the steroids.
- Antiarrhythmic drugs: Enzyme-inducing antiepileptic agents are known to increase the metabolism of amiodarone, disopyramide, mexiletine, and quinidine, thereby necessitating an increase in the dosage of the antiarrhythmic drugs (Patsalos and Perucca, 2003).
- Anticoagulants: Co-administration of direct oral anticoagulants like dabigatran, rivaroxaban, apixaban, and edoxaban with antiepileptic drugs like levetiracetam and valproic acid is believed to increase the risk of thrombotic events, according to a 2023 article by Candeloro et al., published in the journal Research and Practice in Thrombosis and Haemostasis, titled “Drug-drug interactions between direct oral anticoagulants and anticonvulsants and clinical outcomes: A systematic review.” However, the authors clarify that more large-scale research studies need to be undertaken before an association is conclusively proven.
Are antiepileptic agents addictive?
Yes, specific formulations of antiepileptic agents are addictive and known to cause physical dependence and withdrawal. For instance, phenobarbital is known to cause physical dependence in a subset of epilepsy patients.Growing evidence points to the abuse potential of new antiepileptic agents. For instance, pregabalin in supratherapeutic doses produces a “high,” which is the reason for the drug being widely abused.
Psychological dependence on antiepileptic agents is rarely observed in patients. Physical addiction is accompanied by the development of tolerance to the anticonvulsant effects of the drug and the manifestation of withdrawal symptoms when the drug is stopped abruptly or its dose reduced.
What happens if you take too much antiepileptic agents?
If you take too much antiepileptic agents, you are likely to experience lethargy, loss of muscle coordination that affects balance and speech, rapid and uncontrolled eye movements, and altered consciousness. Overdosing on antiepileptic medications that act by blocking sodium channels produces adverse effects like seizures and abnormal cardiac activity. Those agents that act on multiple pathways tend to produce toxicity symptoms that affect multiple organs. In severe cases, taking too much antiepileptic agents causes respiratory depression, leading to coma and death.
